ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Laparoscopic Myotomy and Fundoplication for Achalasia
Patient Selection
Patients should be evaluated to confirm the diagnosis of primary achalasia. While a barium swallow can suggest the diagnosis, confirmation is best obtained with a motility study. In addition to confirming the diagnosis, the lower esophageal sphincter pressure measured on preoperative motility studies has been correlated with outcome after myotomy for achalasia (USC unpublished data). Although uncommon, some patients with achalasia also have a hiatal hernia, and the presence or absence of a hernia should be determined with a barium swallow or upper endoscopy. Prior therapy with balloon dilatation or Botox injection can make the myotomy more difficult, but does not represent a contraindication to a laparoscopic procedure. Typically a myotomy with Dor hemifundoplication is performed for patients without a hiatal hernia, while reduction of the hernia, crural closure and Toupet hemifundoplication is preferred for patients with a hiatal hernia.
Operative Steps
Patients should be placed on a liquid diet several days prior to the procedure to minimize residual debris within the esophagus, both to limit contamination in the event of a mucosal injury and to reduce the potential for aspiration during induction of general anesthesia. We keep the back of the operating table elevated a minimum of 45º while intubating patients with achalasia to further minimize the potential for aspiration during induction and intubation.
 |
| Figure 1 |
After intubation the patient is placed in the lithotomy position with reverse Trendelenburg. A total of five ports are placed in positions similar to those for a laparoscopic Nissen fundoplication, and a 30 degree camera is used (Figure 1). In patients without a hiatal hernia a minimum of dissection is done around the hiatus. The gastro-hepatic omentum is incised and the right crus is identified (Video 1). Next, by pushing the esophagus posteriorly the phrenoesophageal ligament is exposed and elevated. It is then divided towards the left to expose the left crus (Video 2). The gastroesophageal junction fat pad is excised while the left (anterior) vagus is dissected and retracted to the right (Video 3). The line of the myotomy is marked with cautery, and is positioned well over on the left side of the esophagus. The myotomy is initiated a centimeter or two above the gastroesophageal junction in what is the thickest area of the lower esophageal sphincter. Using the hook cautery the outer longitudinal and inner circular muscle layers are divided and the mucosa is exposed (Video 4). The myotomy is extended proximally until the muscle layers thin to normal, usually 5-6 cm above the gastroesophageal junction. Next, the myotomy is extended distally for a minimum of 2 cm onto the stomach along the greater curve side to divide the sling fibers at the angle of His (Video 5). Separation of the muscle layers from the mucosa becomes more difficult on the stomach, and care must be taken to avoid mucosal injury. However, an inadequate myotomy distally is probably the most common cause for incomplete myotomy necessitating reoperation [1]. The mucosa in the area of the myotomy can be checked for a leak by passing an endoscope or a nasogastric tube and insufflating air with the esophagus under water or saline.
Note: RealMedia videos currently unavailable.
 |
 |
| Video 1 | Video 2 |
 |
 |
| Video 3 | Video 4 |
 |
 |
| Video 5 | Video 6 |
After completion of the myotomy the muscle edges are pushed apart using a laparoscopic peanut dissector (Video 6), and hemostasis is achieved with Surgicel or other topical procoagulant. The use of cautery on the mucosa should be avoided to minimize the risk of delayed perforation. A suitable Dor fundoplication can be created in most patients without needing to take down any short gastric vessels, although if mobility of the fundus is restricted the uppermost short gastric vessels should be divided. The anterior fundus is sutured to the left crus and the left edge of the myotomy (Video 7a). It is then brought over to cover the myotomy and sutured to the right crus and the right edge of the myotomy (Video 7b).
 |
 |
| Video 7a | Video 7b |
In patients with a hiatal hernia the right and left crura are identified and the esophagus dissected circumferentially to expose the hiatus posteriorly. The hernia is reduced and the crura approximated with non-absorbable sutures. Short gastric vessels and the posterior pancreatic-gastric vessels are divided to completely mobilize the fundus and create a sufficiently large window posterior to the esophagus for the posterior fundus to pass through easily. Subsequently, the gastroesophageal junction fat pad is removed, the anterior vagus retracted to the right, and the myotomy performed as described above. The posterior fundus is then brought behind the esophagus and sutured to the right crus of the diaphragm and the right edge of the myotomized esophageal muscle. Lastly, the anterior fundus is sutured to the myotomized left muscle edge and to the left crus at the hiatus. This technique distracts the myotomy edges apart and may help prevent restenosis from occurring, but leaves the mucosa uncovered (Figure 2).
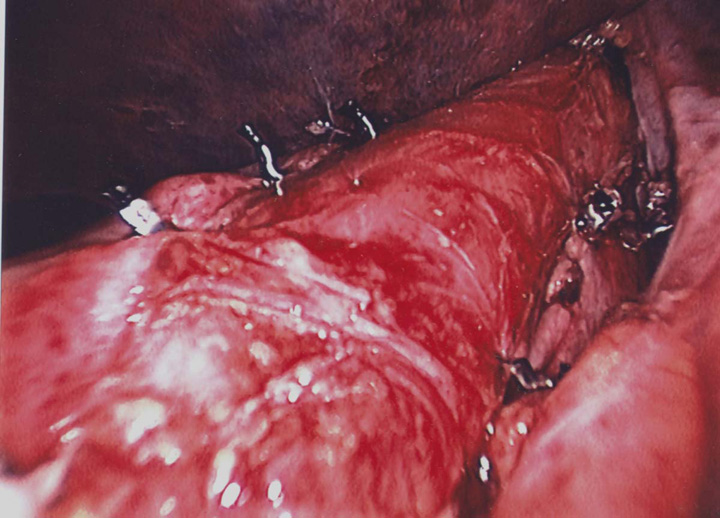 |
| Figure 2 |
Mucosal injuries during myotomy are more likely to occur in patients with prior therapy for achalasia, particularly Botox injection, and should be repaired with fine absorbable monofilament suture such as 4-0 PDS [2]. Rarely is a mucosal injury cause for conversion to an open procedure, but consideration should be given to covering the area of the myotomy with the fundus either using a Dor procedure or by modifying the position of the Toupet so that the anterior fundus covers the myotomy. If a mucosal injury has occurred, it is suggested that a Gastrografin swallow be obtained on the first or second day prior to institution of oral feeding, and fever or clinical signs of infection should precipitate urgent Gastrografin swallow or upper endoscopy to evaluate the possibility of esophageal leak in any patient after myotomy regardless of whether or not the mucosa was known to be violated. Small leaks are frequently missed on a Gastrografin swallow, so a high index of suspicion and early use of endoscopy should be part of the evaluation of patients with symptoms and signs consistent with possible perforation or leak.
 |
| Video 8 |
Visualization with current laparoscopic cameras is excellent; however, the 3-D view using the Intuitive da Vinci robot provides a truly spectacular image during the myotomy. Further, the articulating wrist with hook cautery can facilitate performance of the procedure (Video 8). The precision, high magnification, and 3-D optics of the Intuitive da Vinci robot may reduce the incidence of mucosal injury associated with myotomy, particularly in patients with fibrosis after prior therapy for their achalasia.
Preference Card
- 30º laparoscope
- Bladeless trocars (5 and 10 mm)
- Curved 5 mm endo-shears
- Endo peanut dissectors
- 2-0 silk for fundoplication
- 0 braided non-absorbable suture for crural closure
- 4-0 monofilament absorbable suture for mucosal repair
Tips & Pitfalls
- Take every precaution to prevent aspiration during induction of anesthesia.
- Minimize dissection around the esophageal hiatus unless a hiatal hernia is present. Keep the operative field dry particularly during the myotomy to optimize visualization, but avoid using cautery on the mucosa.
- Place the myotomy on the left side of the esophagus.
- Using the hook cautery, lift the muscle well up off the mucosa and apply the current intermittently to prevent excess heat transfer to the mucosa.
- A laparoscopic peanut dissector can help develop the plane once the mucosa is identified.
- Avoid injury to the anterior vagus nerve particularly near the top of the myotomy where the nerve crosses over to the left side of the esophagus.
- Make sure the myotomy is complete, particularly distally onto the stomach.
Results
Most patients take clear liquids on the day after surgery and notice a dramatic improvement in their swallowing. Patients should be maintained on soft solids for several weeks to allow the edema of the fundoplication to resolve and prevent injury to the mucosa. A regular diet can be resumed after about 4 weeks. Follow-up with a timed barium swallow is the best method to document the promptness and completeness of esophageal emptying post myotomy, and may indicate those most likely to do well long-term [3].
References
- Oelschlager BK, Chang L, Pellegrini CA. Improved outcome after extended gastric myotomy for achalasia. Arch Surg 2003;138:490-5.
- Horgan S, Hudda K, Eubanks T, et al. Does botulinum toxin injection make esophagomyotomy a more difficult operation? Surg Endosc 1999;13:576-9.
- Kostic SV, Rice TW, Baker ME, et al. Timed barium esophagogram: A simple physiologic assessment for achalasia. J Thorac Cardiovasc Surg 2000;120:935-46.



