
Introduction
Intrathoracic goiters are encountered less often today than they were in previous decades. Nonetheless, they are still considered a diagnostic possibility in all anterosuperior mediastinal masses, particularly in Eastern Europe and Asia. Creswell and Wells [1] in 1992 reported that intrathoracic thyroid masses accounted for 5.8% of all mediastinal masses. For an intrathoracic thyroid, surgical removal is indicated when the mass is large, when there is local compression of adjacent structures, and when there is a possibility of malignancy. This can be performed through the neck or by the addition of a partial or complete sternotomy if necessary.
Patient Presentation
A 58-year-old Chinese man presented with a dry cough of three months’ duration. A chest x-ray at a local hospital revealed "a shadow in the superior mediastinum." A subsequent CT scan suggested "ectopic intrathoracic thyroid" (Figures 1 and 2). His physical examination revealed normal temperature and heart rate, without any signs of hyperthyroidism. Palpation of the neck revealed a non-tender, firm, fixed, and non-pulsatile 2 cm right inferior thyroid mass. A repeat chest x-ray confirmed a mass in the right anteromedial mediastinum, with smooth margins, tracheal compression, and deviation of the trachea to the left (Figure 3). Nuclear Tc99 thyroid scan revealed a cold nodule in the right inferior thyroid gland extending below the sternum (Figure 4). The values of total thyroxin 3 (TT3), total thyroxin 4 (TT4), free thyroxin 3 (FT3), free thyroxin 4 (FT4), and thyroid stimulating hormone (TSH) were all normal. Due to the suspicion of malignancy and to avoid the development of tracheomalacia, surgery was performed to remove the mass.
 |
 |
| Figure 1: The arrow indicates the middle mediastinal mass. | Figure 2: The arrow indicates the right middle mediastinal mass, trachea compressed. |
 |
 |
| Figure 3: The arrow indicates the right upper mediastinal mass, trachea compressed. | Figure 4: The arrow indicates the “cold” mass of right inferior thyroid that extends into the thorax. |
Operative Procedure
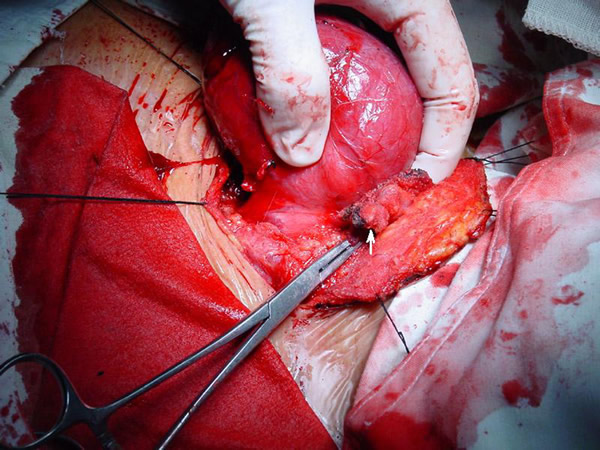
At operation, through a cervical collar incision 2 cm above the supra-sternal notch, and with the neck extended, the right thyroid gland was explored. The right thyroid gland extended into the middle mediastinum posterior to the innominate vein and lateral to the trachea. The mass was completely encapsulated and hyper-vascular. First, the right middle thyroid vein was ligated and divided, allowing easier access to the intra-thoracic mass. The mass was gently extracted by careful blunt dissection from the mediastinum (Figure 5). The right inferior thyroid vein and artery were exposed, ligated, and divided. Parathyroid glands were not identified. The mass was subsequently removed, preserving the superior portion of the right thyroid gland, and measured 8 x 6 x 5 cm (Figure 6). The recurrent laryngeal nerve was protected during the operation. The wound was closed in layers with a drain in place. The patient was extubated in the operating room and remained stable with no respiratory stridor or airway compromise. The postoperative course was uneventful with no hoarseness, dyspnea, or hypocalcemia (Figure 7). The pathological diagnosis confirmed a benign thyroid adenoma.
 |
 |
 |
| Figure 5: The arrow indicates the right superior thyroid vessels being clamped. | Figure 6: Operative specimen – intra thoracic thyroid gland. | Figure 7: The postoperative wound. |
Discussion
Wakeley and Mulvany [2] in their 1940 seminal report divided intrathoracic thyroid into three types: (a) "small substernal extension" of a mainly cervical thyroid goiter; (b) "partial" intrathoracic goiter, in which the major portion of the goiter is situated within the thorax; (c) "complete" intrathoracic goiter, in which all of the goiter lies within the thoracic cavity. With an overall incidence of 8.7% for substernal goiters, the incidences of the three types were 81.9%, 15.3%, and 2.7%.
Ectopic intrathoracic thyroid is a rare presentation of thyroid disease and of all mediastinal tumors [3]. It is defined as the presence of enlarged thyroid tissue below the plane of the thoracic inlet. Utilizing the Shield’s classification of the mediastinum [4], they are mostly located in the anterior and middle mediastinum, and rarely in the posterior mediastinal compartment [5] [6]. The majority are located in the middle mediastinum, and they descend along the trachea into the mediastinum. This is the reason for their common association with tracheal compression and deviation. One third of patients are asymptomatic. Commonly observed symptoms include cough, dyspnea, stridor, and dysphagia [7][8]. The symptoms are typically caused by tracheal compression, and an intrathoracic or mediastinal component is present in more than 75% patients with compression [9]. Leuchter et al. [10] reported a rare association with Horner's syndrome. A mass surrounding the trachea in the middle mediastinum on chest x-ray, CT scan, and nuclide scan, suggests the diagnosis.
For a multinodular goiter with compression symptoms occurring with an intrathoracic component, surgery offers definitive treatment [9]. Other indications for surgery include an abnormal fine-needle biopsy, progressive thyroid enlargement, thyrotoxicosis, and superior vena cava syndrome [4]. Intra thoracic thyroid disease, with rare exceptions, can be resected through a cervical collar incision [11]. This approach is adequate in the majority of cases, since the blood supply from the superior and inferior thyroid arteries originates in the neck [12]. The basic operative steps of thyroidectomy have been described by Shaver and Clark [13]. Sternotomy, partial sternotomy, and right anterior thoracotomy are most frequently needed for treatment of intrathoracic thyroid carcinoma as they offer greater exposure and access for radical excision and control of intraoperative bleeding that may occur in the mediastinum [14]. Postoperative complications include transient hypocalcemia, recurrent laryngeal nerve injury, bleeding, wound infection, and tracheomalacia. If tracheomalacia is thought to be a significant risk, intraoperative tracheotomy or T-tube placement should be performed prior to extubation in the operating room. However it is difficult to to detect tracheomalacia prior to resection[15]. Hedayati et al [5] report that parathyroid devascularization is more common with resection of a substernal goiter and autotransplantation can prevent permanent hypoparathyroidism. A cervical approach for definitive resection remains the mainstay of management of the intrathoracic thyroid at this time.
References
- Creswell LL, Wells SA. Mediastinal masses originating in the neck. Chest Surg Clin N Am 1992;2:23-55.
- Wakely CPG, Mulvaney JH. Intrathoracic Goiter. SGO 1940;70:703. Shields, TW. General Thoracic Surgery. 2005. Sixth Edition. Chapter 168, 2500-2512
- Sakorafas GH, Vlachos A, Tolumis G, Kassaras GA, Anagnostopoulos GK, Gorgogiannis D. Ectopic intrathoracic thyroid: case report. Mt Sinai J Med 2004;71:131-133.
- Shields TW. The Mediastinum, Its Compartments, and the Mediastinal Lymph Nodes. Shields, TW. General Thoracic Surgery. 2005. Sixth Edition. Chapter 154, 2343-2346
- Hedayati N, McHenry CR. The clinical presentation and operative management of nodular and diffuse substernal thyroid disease. Am Surg 2002;68:245-52.
- Adegboye VO, Ogunseinde OA, Obajimi MO, Ladipo JK, Brimmo AI. Pattern of intrathoracic goiter in Ibadan, Nigeria. Niger Postgrad Med J 2002;9:226-232.
- Ignjatovic M, Stanic V, Cuk V, Kostic Z. Intrathoracic goiter: analysis of 21 cases. Acta Chir Iugosl 2002;49:15-25.
- Tsukada H, Kojima K, Takeuchi S, Osada H. Intrathoracic retroesophageal goiter causing tracheal stenosis. Jpn J Thorac Cardiovasc Surg 1999;47:174-177.
- Rios A, Rodriguez JM, Canteras M, Galindo PJ, Tebar FJ, Parrilla P. Surgical management of multinodular goiter with compression symptoms. Arch Surg 2005;140:49-53.
- Leuchter I, Becker M, Mickel R, Dulguerov P. Horner's syndrome and thyroid neoplasms. ORL J Otorhinolaryngol Relat Spec 2002;64:49-52.
- Houck WV, Kaplan AJ, Reed CE, Cole DJ. Intrathoracic aberrant thyroid: identification critical for appropriate operative approach. Am Surg 1998;64:360-362.
- Kucharczuk JC, Shrager JB. Anterior Mediastinal Masses. In Sellke FW, del Nido PJ, Swanson SJ, et al. Sabiston & Spencer Surery of the Chest, Vol I. Philadelphia, PA, Elsevier, 2005. 675
- Shaver JK, Clark OH. Chapter 4, Surgery for Neoplasms of the Thyroid gland. In Bland KI, Karakousis CP, Copeland EM, et al. Atlas of Surgical Oncology. Philadelphia PA, WB Saunders, 1995; 129-144.
- Nervi M, Iacconi P, Spinelli C, Janni A, Miccoli P. Thyroid carcinoma in intrathoracic goiter. Langenbecks Arch Surg 1998;383:337-339.
- Maddaus MA, Pearson FG. Tracheomalacia. In Pearson FG et al ed. Thoracic Surgery. 2nd edition, New York, Churchill Livingstone. 2002; 320-325.



