ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Single Incision Minimally Invasive Cardiac Surgery (SIMICS)
By Theodore Kofidis, MD, PD, Duc Thang Vu, MD, Lian-Kah Ti, MD, Edgar Tay, MBBS, Lee Chuen Neng, MD
Background
Minimally invasive cardiac surgery (MICS) is on the march and is becoming state of the art for a series of cardiac procedures [1]. With the advent of hybrid therapies, it even promises to play a dominant role in the Cardiac Surgeons' and Cardiologists' armamentarium in the future. Although the term "Minimally Invasive" is often being used euphemistically and with variable content, it is now well known that it bears substantial advantages, such as reduced length of stay, faster recovery, less trauma, better cosmetic result and in some cases, less surgery related complications, such as hemorrhage and infection [2].
Minimally invasive mitral valve surgery is employed in many advanced centers around the globe with interesting variations. For the sake of a small lateral incision vs. a full median sternotomy, a number of small incisions and ports need to be fashioned to allow for entry of endoscopic tools, cameras and aortic cross-clamps. An additional femoral incision is usually performed for femoral cannulation and cardiopulmonary bypass (CPB). As a result, the patients' torso is being penetrated at various spots and the "minimally invasive" term for the procedure is questionable (figure 1).
In the past few years some instrumental innovations emerged, aiming at reducing trauma to the patient. For instance, the Glauber clamp is a fully insertable and deployable aortic crossclamp that was designed by Mattia Glauber, an Italian Cardiac Surgeon, and produced by Sorin Group Inc [3]. It comes in three sizes to fit all chest anatomies; small, medium and large. Other types of clamps are malleable and exit the chest through the work port. However, their disadvantage is that they occupy significant space and are "in the way". The Intraclude™ (Edwards Lifesciences, Irvine, USA) device, formerly known as Endoclamp may also save a port [4]. Its updated version causes less complications, features a different balloon shape and consistency as well as improved coating. In the largest reported series, published by Van Praet et al, it has proven a useful tool in first time as well as redo surgeries, both valve and redo-CABG [5].
Here, we describe our first experience with a new surgical approach, utilizing new technologies, as well as custom-made tools to achieve minimally invasive open heart valve surgery through one single working port, and omit all the rest (ports for CO2, Suction, Camera, Cross-clamp, Cannulation). We introduced a novel procedure of minimally invasive heart valve surgery, which we call Single Incision Minimally Invasive Cardiac Surgery (SIMICS).
Patient Selection
The first patient was a 48 years old Australian male, following endocarditis and accomplished antibiotic regimen. In addition, 12 weeks before surgery the patient was comatose as a result of cerebral complications due to endocarditis as well as alcohol- encephalopathy and liver cirrhosis with severe and prolonged seizures. He recovered well, even though cachectic, without functional neurological deficits, and walked in our preoperative outpatient clinic in a fully oriented and coherent state.
Patients with known severe peripheral vascular disease should not be considered for this procedure.
In addition, a variety of procedures should be feasible in the same setting: tricuspid valve repairs/replacements, MAZE procedures, ASD closures, intra-atrial tumor removals, redo procedures and others. The utilization of the currently existing pre-closing devices should be expanded following more extensive studies.
Operative Steps
1. The patient was positioned the usual way for MICS surgery, i.e. left 150 rotated supine position with exposure of the axillary and femoral regions. We started with a 5 cm right anterolateral thoracotomy in the 4th intercostal space (ICS), lateral to the nipple (figure 2). The right lung was deflated via double lumen intubation.
2. At this point Heparin was administered and our team cardiologist inserted preclosing sutures in to right femoral artery and vein using the Perclose ProGlide™ vascular closure system (Abbott, Illinois, U.S.A) (Figure 3), deploying the system twice for every vessel. Following femoral cannulation using Seldinger technique, CPB was commenced.
3. We proceeded to open and suspend the pericardium (2 x 2 sutures anteriorly and posteriorly respectively). A further retraction suture was placed at the base of the right atrium, right above the interatrial groove, for additional exposure, as it has proven very efficient at the end of the procedure, for better left atrial closure, following removal of the left atrial lift retractor. All illumination was provided by external lights (Operating theatre lamps and headlights), without any compromise of vision. Next, the cardioplegia line was inserted through the working incision.
4. The next step was the deployment of the Glauber clamp and cardioplegic cardiac arrest (Figure 2a). The left atrium was opened and evacuated from blood through a drop vent. Next, our custom-made atrial retractor (figure 4) was bent to fit in the left atrial curvature and size, the sutures passed through the septum and out the right atrial auricle, to then be "fished" out of the chest cavity and suspended with clips or around the wound retractor (Figure 2b).
5. The repair/replacement procedure was then carried out in the usual fashion, following by rewarming, left atrial closure, deairing, removal of crossclamp, and echocardiographic control (figure 5a). At this point our team cardiologist scrubbed in again to help remove the femoral cannulas and secured hemostasis in the femoral artery and vein using the Perclose ProGlide™ vascular closure system.
6. The chest was closed, and a 24Ch chest tube was inserted through the dorsal part of the working incision (figure 5b). Postoperative care followed the protocol for standard MICS.
Tips & Pitfalls
In order to keep a safety margin, we used the ProGlide™ and utilized a small femoral arterial cannula (18-20 French), which is still sufficient to maintain adequate CPB flows. Further studies involving preoperative Duplex evaluation of the femoral arteries under consideration of weight, size and CPB flow will – and have to- follow.
Extreme anatomy, such as very flat-chested patients, patients with pectus excavatum, vertical mediastinal anatomy should be excluded from this procedure. Latter is because in such cases the heart may either collapse towards the left side, or the mitral valve position itself behind the atrial fold in a cranio-caudal orientation, thereby escaping direct view.
Discussion
Single Incision Minimally Invasive Cardiac Surgery (SIMICS) is our effort to render MICS heart valve surgery even less invasive and omit a series of ports and holes in the chest and groin in which we conceptualized and carried out an operation through one single 5-6 cm working entry on the anterolateral aspect of the chest, using equipment, which is currently on the market, except from a simple, custom-made left atrial lift retractor. The omission of the camera trocar and port in this approach may be viewed as a disadvantage of the procedure we introduce, particularly in educational terms, as the opportunity to follow the procedure from a fixed vision source is abandoned. However, it can be justified in the interest of less invasiveness and postoperative pain. Moreover, the camera occupies an annoying amount of space during the MICS procedure, on the surgeon's left side, often compromising his comfort. Also, it often needs to be readjusted and de-fogged, which is also a disturbing fact. Alternatively, a headlight-mounted camera may prove efficient instead. Presently, we are developing an insertable, small-size camera in a separate study.
The procedure we introduce here, allows for a truly less invasive heart valve surgery, and for omission of unnecessary holes and incisions, which have frequently generated controversy in the past, as for the value and true advantage of MICS surgery. The Single Incision MICS we introduce here may be a valid, improved platform of MICS surgery with eventually better patient satisfaction, cosmetic result and surgical trauma. It may prove an appealing alternative in the hands of committed and experienced MICS surgeons.
Figures
Figure 1: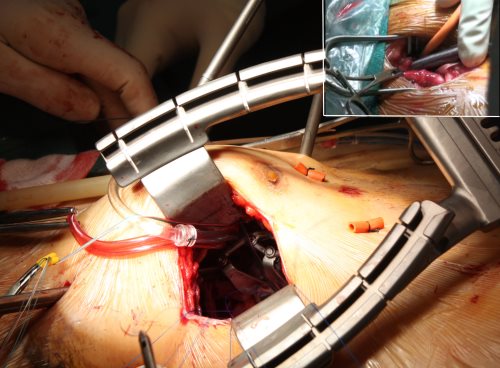
Many holes are required for ports placement in minimally invasive mitral valve surgery.
Figure 2: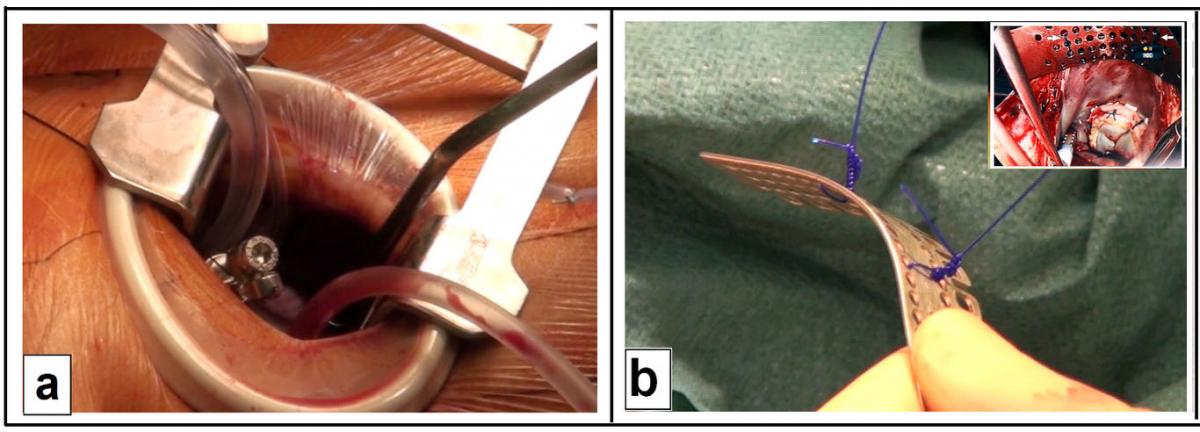
The lateral thoracic incision showing the deployed Glauber clamp (a). Left atrium is open and the atrial retractor (b) is reshaped and positioned in the left atrium (small insert).
Figure 3: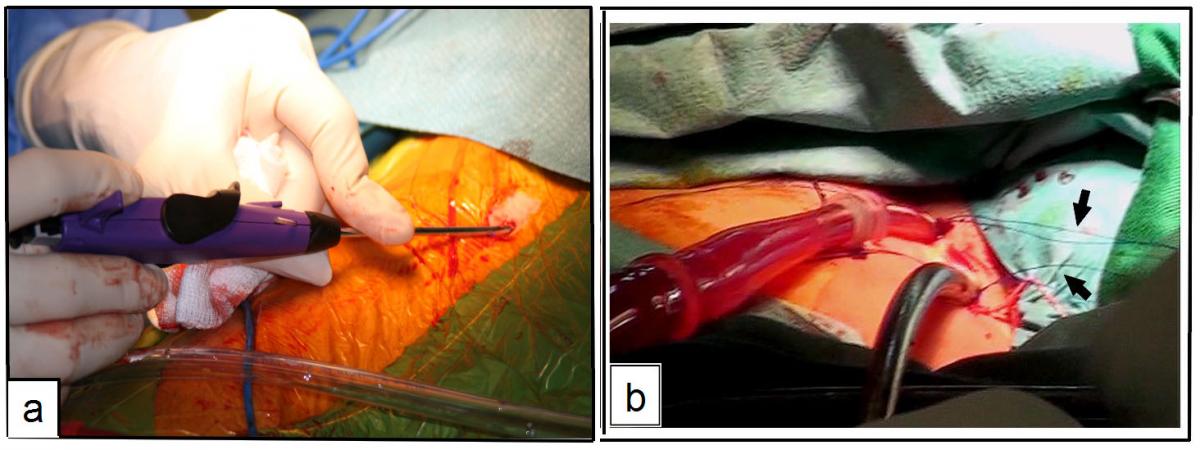
The femoral cannulation starts with vessel preparation by ProGlide device (a), and followed by cannulas insertion (b).
Figure 4:
Some instruments used for single incision minimally invasive cardiac surgery include a) an atrial retractor, b) Perclose ProGlide device, and c) the Glauber clamp.
Figure 5: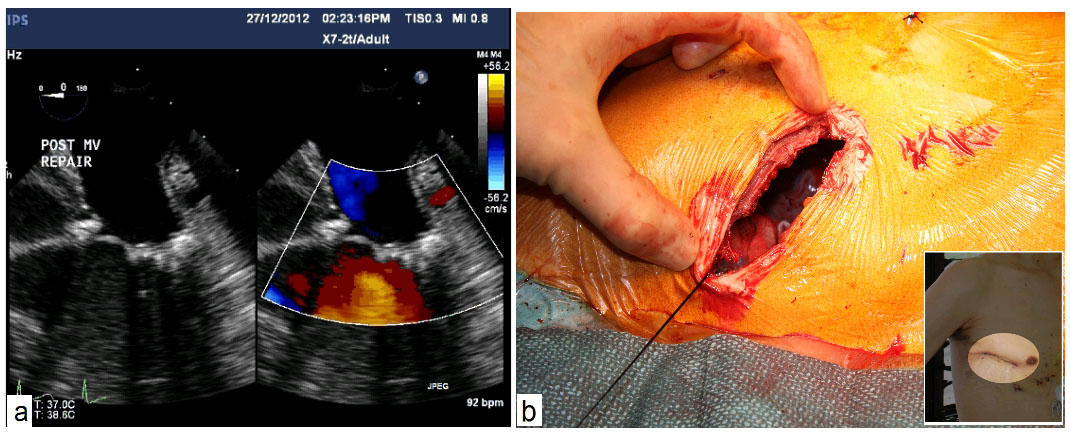
Postoperative echocardiography shows good repair results (a) and a single small chest scar after surgery (b)
References
- Balaguer JM, Umakanthan R, Leacche M, Byrne JG. Minimally invasive cardiac surgery. Curr Probl Surg 2012; 49: 529-549
- Modi P, Rodriguez E, Hargrove WC, 3rd et al. Minimally invasive video-assisted mitral valve surgery: a 12-year, 2-center experience in 1178 patients. J Thorac Cardiovasc Surg 2009; 137: 1481-1487
- Glauber M, Karimov JH. A completely detachable aortic clamping instrument for minimally invasive cardiac surgery. Innovations (Phila) 2010; 5: 309-310
- Ius F, Mazzaro E, Tursi V et al. Clinical results of minimally invasive mitral valve surgery: endoaortic clamp versus external aortic clamp techniques. Innovations (Phila) 2009; 4: 311-318
- Schroeyers P, Wellens F, De Geest R et al. Minimally invasive video-assisted mitral valve surgery: our lessons after a 4-year experience. Ann Thorac Surg 2001; 72: S1050-1054
- Ramponi F, Yan TD, Vallely MP, Wilson MK. Total percutaneous cardiopulmonary bypass with Perclose ProGlide. Interact Cardiovasc Thorac Surg 2011; 13: 86-88
- Kofidis T, Lee CN. A novel and simple atrial retractor. Ann Thorac Surg 2011; 91: 1634-1635



