ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Exposure of the cervical esophagus

Patient Selection
Exposure of the esophagus in the neck is required when an esophagectomy is being performed with a cervical anastomosis. Open three field esophagectomy, transhiatal esophagectomy and minimally-invasive three-field esophagectomy are examples. Exposure for a cervical esophagostomy, open repair of a Zenker’s diverticulum, malignancies of the cervical esophagus and penetrating injuries of the neck resulting in esophageal perforation are less frequent indications for cervical exposure. The preoperative workup is for the underlying condition, as exposure of the cervical esophagus has minimal physiologic impact on the patient.
The preferred side of exposure is the left, as the recurrent nerve is less likely to be injured than on the right due to differences in position and course. The reason for this relates to the position of the left recurrent laryngeal nerve, which is longer and more vertical in position than its counterpart on the right because of its course around the aortic arch rather than the subclavian artery. This decreases the chance of direct injury, as it stays in the tracheoesophageal groove for the majority of its course in the operative field rather than traversing the space between the laryngotracheal complex and carotid sheath. The risk of stretch injury is also decreased, as its length distributes any superior traction forces over a longer segment of nerve.
A short neck, obesity and an enlarged thyroid gland are not contraindications to exposure of the esophagus in the neck. Previous surgery, radiation, and tracheostomy make the dissection more difficult but are not contraindications to exposing the esophagus in the neck.
Operative Steps
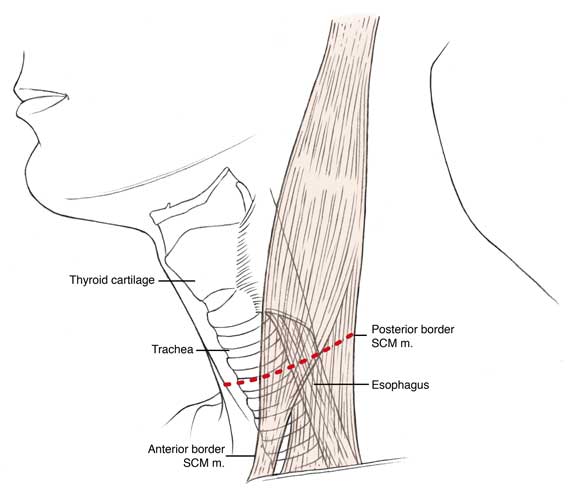 |
| Figure 1: Neck incision for exposure of the cervical esophagus. |
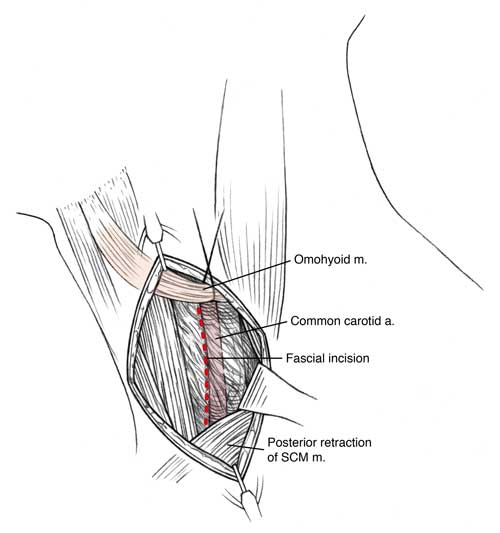 |
| Figure 2: Fascial incision along anterior border of sternocleidomastoid. |
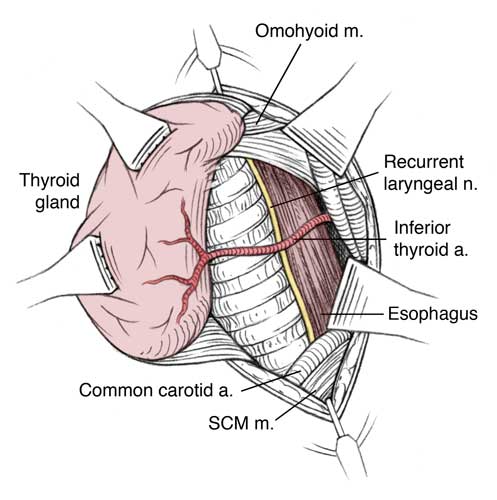 |
| Figure 3: Relation between recurrent laryngeal nerve and inferior thyroid artery. |
- The incision is made horizontally beginning anteriorly at the midline running over the anterior border of the sternocleidomastoid (SCM) muscle and running to its posterior border. It should be located just below level of the cricoid cartilage or two fingerbreadths above the head of the clavicle (Figure 1). Although a more vertical incision along the anterior border of the SCM of equivalent length offers more exposure than a horizontal incision, the cosmesis of the latter is preferable. In situations where exposure is anticipated to be difficult, a more vertical incision may be performed.
- Short subplatysmal flaps are elevated superiorly and inferiorly using cautery and blunt dissection to expose the fascia, which is then incised along the anterior border of the SCM from the clavicle to the level of the thyroid cartilage notch. These flaps are retracted using fish hook retractors that are clamped to the drapes (Figure 2).
A generous incision of this fascia and posterior mobilization of the SCM muscle bluntly allows maximal exposure and makes the field as shallow as possible.
- A self retaining weitlaner retractor is used to maintain the exposure. In the difficult neck it is useful to incise or divide the sternal head of the SCM, which helps mobilize it inferiorly. The SCM muscle is dissected posteriorly off the underlying sternohyoid muscle until the lateral surface of the internal jugular vein is well seen. The anterior belly of the omohyoid muscle is identified, which can be mobilized superiorly or divided as needed for exposure.
- The middle layer of the deep cervical fascia is incised using tenotomy scissors vertically along the anterior border of the internal jugular vein (taking the middle thyroid vein between ligatures of 4-0 silk) and then more deeply (and slightly anteriorly) along the common carotid artery. The carotid sheath can be retracted laterally with an army/navy or Richardson retractor (Figure 2). Placing 2 Allis clamps on the lateral border of strap muscles allows the laryngotracheal complex to be rotated anteriorly and medially, a maneuver which protects the recurrent nerve from traction injury.
- The middle layer of the deep cervical fascia, which surrounds the thyroid/laryngotracheal complex, sends investments to the carotid sheath, which must be divided sharply to allow for entry into the retropharyngeal /paraesophageal space. The inferior thyroid artery (Figure 3) is ligated with 4-0 silk where it courses medially from behind the carotid artery. The distal branches of the inferior thyroid artery intertwine with the recurrent laryngeal nerve; that if the artery is left intact, the traction on it produced by lateral traction on the carotid sheath and medial retraction/rotation of the laryngotracheal complex may pull the nerve out of the groove and increase the chance of injury to it.
If the patient has not been previously operated upon, the recurrent laryngeal nerve is not specifically identified and dissected, as its course (on the left) in the paratracheal groove keeps it away from direct injury if certain principles are adhered to (see below) and the surrounding tissues protect it from direct trauma by retractors and to some degree from stretch injury. If the right side is chosen for exposure, dissection is kept lateral, at the medial aspect of the common carotid artery. The nerve should be identified as it traverses the gap between the carotid sheath and laryngotracheal complex (C7-T1) to go around the subclavian artery (Figure 3).
- The lateral aspect of the left thyroid lobe is grasped with two Babcock retractors and the laryngotracheal complex is rotated anteriorly and medially to expose the lateral and posterior aspect of the pharynx and esophagus. This direction of retraction is well tolerated. To prevent stretch injury to the recurrent laryngeal nerve, superior retraction must be specifically avoided (Figure 4). Although occasionally in the short/fat neck inferior sectioning of the sternohyoid / sternothyroid muscles is necessary for superior displacement of the laryngotracheal complex and esophageal exposure, in general preservation of these muscles helps guard against overly aggressive superior retraction and stretch injury to the recurrent laryngeal nerve.
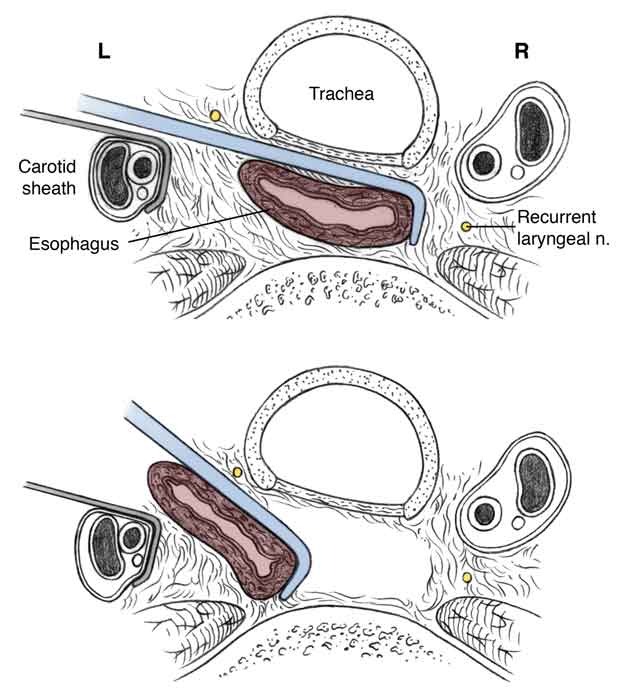
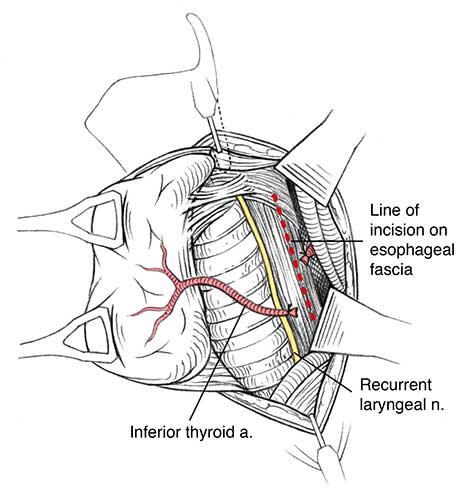 |
| Figure 4: Incision of fascia over the esophagus. |
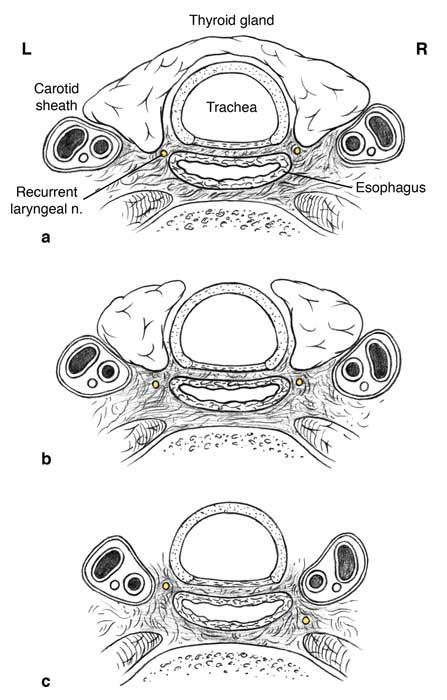 |
| Figure 5: Relation and course of the recurrent laryngeal nerves in the neck at high (a), mid (b) and low (c) levels. |
 |
| Figure 6: Circumferential dissection of the esophagus. |
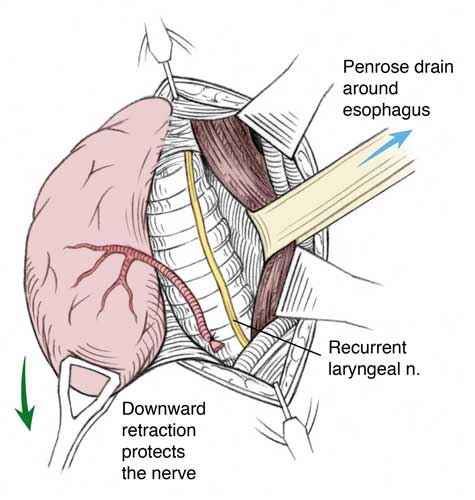 |
| Figure 7: Mobilization of the esophagus. |
- Using the thyroid lobe as a handle on the laryngotracheal complex, because of its tight attachment to it at Berry’s ligament (connective tissue that attaches trachea to thyroid), facilitates exposure without exposing the recurrent laryngeal nerve to direct trauma by a retractor (Richardson or army/navy) where the tip inevitably tends to migrate towards the tracheoesophageal groove where the nerve sits. Alternatively, a hook may be placed along the lateral edge of the thyroid cartilage and used to retract the laryngotracheal complex medially in order to visualize the region of the cricopharyngeal muscle and cervical esophagus.
- With the above exposure, palpate the inferior cornu of the thyroid cartilage, which serves to identify the level of the cricoid cartilage and recurrent laryngeal nerve entry into the larynx. Working 1-2 cm below this, the esophageal fascia is incised sharply on the posterior-lateral aspect of the esophagus vertically downward for a distance of 2-3 cm (Figure 4). Alternatively, the prevertebral plane may be dissected bluntly with a tonsil clamp or peanut dissector to expose the posterior aspect of the esophagus.
Beginning the dissection higher on the esophagus and working on its posterior aspect (4-5 o’clock position) ensures that the recurrent laryngeal nerve is anterior to the plane of dissection and will not be directly injured. Subsequent dissection is done underneath this fascial layer, which protects the nerve from direct injury as it is displaced off the surface of the esophagus. As one proceeds lower in the neck, the left recurrent laryngeal nerve runs more anteriorly, decreasing the chance of direct injury if the dissection is kept on the esophagus (Figure 5).
- Once the subfascial plane is entered, dissection with a right angle clamp, the tip of which hugs the muscular layer of the esophagus, is performed starting posteriorly and proceeding anteriorly, working first behind and then anterior to the esophagus, developing a circumferential plane around the esophagus (Figure 6). Gentle medial retraction on the trachea can facilitate this, as it tends to rotate the esophagus to a more leftward position. Because the dissection is done from left to right and is 3-4 cm below the cricoid cartilage, the right recurrent laryngeal nerve is protected from direct injury, as at this level it has already traversed laterally off the esophagus (Figure 5).
- Using a right angle clamp, a 1” penrose drain is passed around the esophagus. Using this drain, the esophagus is gently retracted laterally and superiorly, and a combination of sharp and blunt (finger/peanut) dissection performed starting superiorly and proceeding inferiorly towards the thoracic inlet to gradually mobilize and dissect the esophagus from the surrounding soft tissues (Figure 7). Care must be taken to avoid injury to the posterior tracheal wall while doing this.
While performing this dissection a critical step is to provide specific downward counter traction on the thyroid lobe to prevent stretch injury on the nerve, which can easily occur if, in the process of retracting the esophagus superiorly, the laryngotracheal complex is pulled up as well. This circumferential dissection of the esophagus can be carried inferiorly into the posterior superior mediastinum when being performed for esophagectomy and superiorly as needed for other operations on the esophagus. When the (thoracic) esophagus is brought up into the neck and transected, specific attention to this downward traction must be maintained to prevent recurrent nerve injury.
Preference Card
- Blunt (fish hook) skin retractors
- Weitlaner retractor
- Bipolar cautery
- Tenotomy scissors
- Babcock retractors
- One inch Penrose drain
Tips & Pitfalls
- Use a headlight and loops to improve visualization.
- Divide inferior thyroid branches
- Rotate the laryngotracheal complex anteriorly and medially by using retraction on the thyroid or strap muscles to maximize the chance to protect the recurrent laryngeal nerve.
Results
Pulmonary complications occur in up to 25% of patients following esophageal resection, and aspiration pneumonia carries the highest risk of death following esophagectomy [1]. Both minimally invasive and traditional esophagectomy carry similar risks of pneumonia (20%) and recurrent laryngeal nerve injury (18%) [2]. Exposure of the esophagus in the neck is often performed by thoracic or general surgeons who do not operate on this part of the esophagus on a daily basis and therefore may not appreciate the maneuvers required to consistently and reliably protect the left recurrent laryngeal nerve during this dissection. Considerable morbidity and subsequent mortality results from injury to the nerve either by traction or transection presenting as inability to generate an adequate cough and aspiration in the postoperative period [3]. Studies demonstrate that 67% of patients following esophageal resection develop swallowing abnormalities which were not present preoperatively [4]. Furthermore, laryngeal penetration and subsequent tracheal aspiration occurred in half of those patients. The pathophysiology of recurrent nerve injury involves vocal fold and pharyngeal dysfunction, as well as cricopharyngeal denervation all of which lead to inability to sufficiently protect the airway. In combination with recurrent nerve injury, damage to the superior laryngeal nerve further exacerbates the situation by the loss of laryngeal sensory input leading to “silent aspiration” occurring in over 70% of patients [5-7].
Several techniques have been proposed to reduce the risk of recurrent nerve injury. Early division of the vagus nerves, careful cervical esophageal dissection; and the avoidance of retractors on the tracheoesophageal groove during the cervical portion of the esophagectomy have been described. We propose additionally that avoidance of superior traction on the thyroid gland is protective of the recurrent nerve.
A detailed description of the technique of exposure of the cervical esophagus is lacking in most modern Thoracic texts and this article attempts to describe how this can be done safely and easily by general thoracic surgeons.
References
- Atkins BZ, et al. Reducing hospital morbidity and mortality following esophagectomy. Ann Thorac Surg 2004:78:1170-6.
- Atkins BZ, Fortes DL, Watkins KT. Analysis of respiratory complications after minimally invasive esophagectomy: preliminary observation of persistent aspiration risk. Dysphagia 2007;22:49-54.
- Bailey SH, et al. Outcomes after esophagectomy: a ten-year prospective cohort. Ann Thorac Surg 2003;75:217-22.
- Heitmiller RF, Jones B. Transient diminished airway protection after transhiatal esophagectomy. Am J Surg 1991;162:442-6.
- Heitmiller RF, Tseng E, Jones B. Prevalence of aspiration and laryngeal penetration in patients with unilateral vocal fold motion impairment. Dysphagia 2000;15:184-7.
- Perie S, et al. Aspiration in unilateral recurrent laryngeal nerve paralysis after surgery. Am J Otolaryngol 1998;19:18-23.
- Setzen M, et al. The association between laryngopharyngeal sensory deficits, pharyngeal motor function, and the prevalence of aspiration with thin liquids. Otolaryngol Head Neck Surg 2003;128:99-102.



