ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Implantation of the Syncrus(TM) Internal Cardioversion System for Postoperative Atrial Fibrillation
Operative Steps
There are 4 wires implanted in the Syncrus™ System.
- Left Atrial Cardioversion wire
- Right Atrial Cardioversion wire
- Right Atrial Pacing wire
- Ventricular Pacing wire
Left Atrial Cardioversion Wire
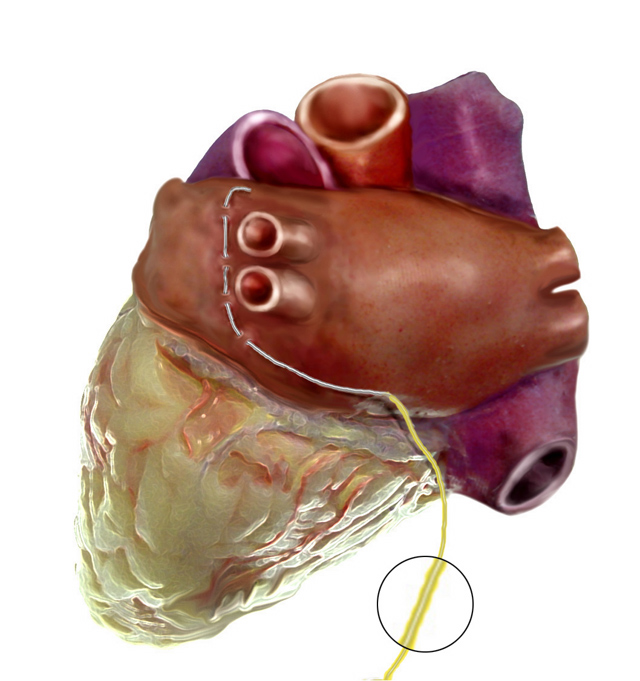
Figure 1. |
Arrested Heart Placement
The left atrial cardioversion wire (yellow) is the first wire to be implanted on the heart. It is placed before the valve repair/replacement or after the distal circumflex grafting is performed. The heart is lifted in order to have adequate exposure of the left pulmonary veins. The wire is attached to the left atrium anterior to and within 5mm of the left superior pulmonary vein. The wire is placed in a linear fashion with 2-4 bites of the atrial epicardium. The needle from the wire is cut and small crimp is made in the distal end of the wire. The wire is then draped over the dome of the left atrium or atrial appendage. This will allow 3 to 5 cm of wire to contact the epicardium. The wire is then brought out through the right side of the chest and secured to the skin with suture. A cardioversion connector is attached to the wire.
Beating Heart Placement
The left atrial cardioversion wire (yellow) is placed first, before the operation is performed. The heart while still beating is lifted anteriorly and rotated to the right of the patient using a suction exposure device. The wire is the placed in a similar fashion described above for the arrested heart.
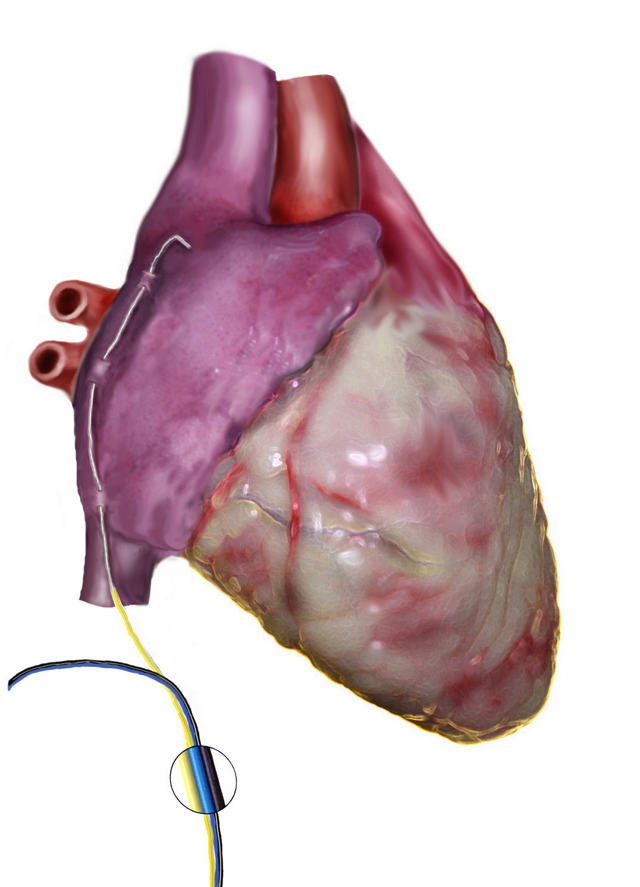
Figure 2. |
Right Atrial Cardioversion Wire Placement
The right atrial cardioversion wire (yellow) is placed at the end of the operation right before or just after the patient is weaned the CPB machine. In the beating heart patient, right after the bypass grafts have been performed, the wire is placed. The wire is placed within 5mm of the SA node linear fashion with 2-4 bites of the atrial epicardium. The needle from the wire is cut and small crimp is made in the distal end of the wire. The wire is then draped laterally along Waterston's Groove down to the inferior vena cava. This will allow 3 to 5 cm of wire to contact the epicardium. The wire is then brought out through the right side of the chest and secured to the skin with suture. A cardioversion connector is attached to the wire.
Right Atrial Pacing Wire Placement
The right atrial pacing wire (black/blue) is placed after the right cardioversion wire. The wire is placed on the atrial appendage. The wire is placed in a linear fashion with 2-4 bites of the atrial epicardium. The needle from the wire is cut and small crimp is made in the distal end of the wire. The wire is then brought out through the right side of the chest and secured to the skin with suture.
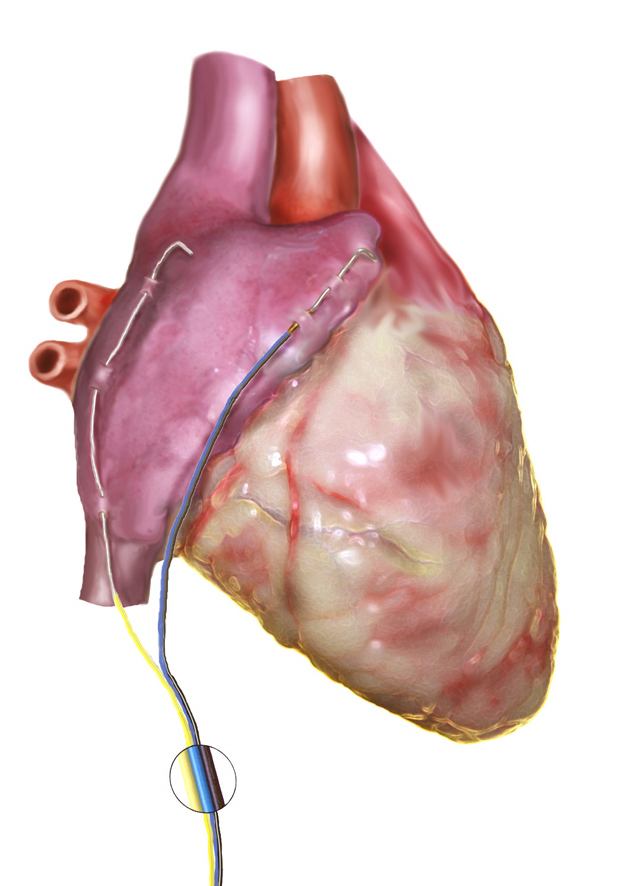
Figure 3. |
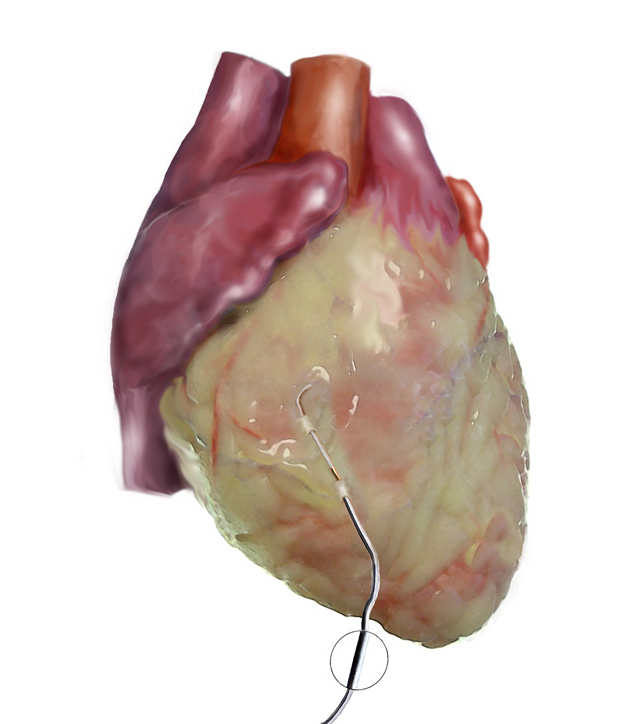
Figure 4. |
Ventricular Pacing Wire Placement
The ventricular pacing wire (black/white) is placed last using the arrested heart or beating heart technique. The wire is placed on the right or left ventricle. The wire is placed in a linear fashion with 2-4 bites of the atrial epicardium. The needle from the wire is cut and small crimp is made in the distal end of the wire. The wire is then brought out through the left side of the chest and secured to the skin with suture.
Tips & Pitfalls
- Syncrus can be placed in all cardiac surgery patients.
- The wires are placed in a linear fashion to maximize contact and decrease the risk of tearing the myocardium during removal.
- Only one atrial and ventricular pacing wire is required because they are bipolar. Both wires are tested for conductivity by a standard dual chamber temporary pacer.
- The cardioversion wires are tested by attaching both of them simultaneously to the atrial lead of the temporary pacemaker. Lead function is adequate if a pacing spike is demonstrated on the electrocardiogram when the pacemaker is set to 10mV
- Other patterns of attachment have been tried but may lead to bleeding on both implantation and removal.
- The left atrial cardioversion wire should not overlap the ventricle, so as to concentrate the energy on the atrium.
- Different locations of placement of the cardioversion wires may reduce the effectiveness and increase the energy requirement to successfully cardiovert.
- Cardioversion wires should be placed on bare myocardium, as epicardial fat may impede energy transfer to the heart
- The wires are removed similarly to standard pacing wires the day before the patients are discharged home.
References
- Kleine P, Blommaert D, van Nooten G, et al. Multicenter results of TADpole heart wire system used to treat postoperative atrial fibrillation Eur J Cardiothorac Surg 1999;15:525-526.
- Liebold A, Haisch G, Rosada B, Kleine P. Internal atrial defibrillation - a new treatment of postoperative atrial fibrillation. Thorac Cardiovasc Surg 1998;46:323-6.



