ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Management of Contained Rupture of Wrapped Ascending Aorta: Redo Sternotomy, Replacement of Aortic Valve, and Ascending Aorta
Raheel F, Efthymiou C, Kahn S, Mariscalco G. Management of Contained Rupture of Wrapped Ascending Aorta: Redo Sternotomy, Replacement of Aortic Valve, and Ascending Aorta. October 2020. doi:10.25373/ctsnet.13146218
Patient Selection
The standard method of treatment for an ascending aorta aneurysm is replacement with the Dacron tube graft. However, some surgeons use alternative techniques in selected cases for dilated ascending aorta, such as wrap without aortoplasty (1, 2), wrapping of the ascending aorta with a fine transparent and stretchable Dacron mesh (3), manually pre-prepared prosthesis which respects the shape of the aorta (4), and reduction aortoplasty with wrapping (5, 6). The Dacron sleeve is another wrapping technique without division of the Dacron tube graft - the original circumference of the Dacron tube graft remains intact, therefore the strength and contour of the Dacron tube graft does not alter (7).
The biomechanical analysis of wrapping the moderately dilated ascending aorta, using the finite elements method, suggested that after a wrapping procedure, the aortic wall is subject to similar stress that occurs in the normal aorta and lower stress than in the nonwrapped moderately dilated aorta (8). In one study, no late aortic complications were detected in the follow-up (median 71.1 months) of the wrapping of the moderately dilated ascending aorta that had aortic valve replacement for bicuspid aortic stenosis (9).
However, splitting and suturing the Dacron tube graft loses its maximum elasticity that was at 45 degrees between the longitudinal and transverse threads (10). This could lead to the thinning and atrophy of the aortic wall (11). The case report of two patients demonstrated that the aortic wall underlying the reinforcement cuff was extremely atrophic, and normal aortic layers lost their existence. Aortic residual showed typical cellular and neovascular infiltration and a foreign body reaction (11). Late rupture after Dacron wrapping of aortic aneurysms was also reported in 1986 (12). Aortic wrap may cause erosion of the aortic wall due to dislocation of the wrap (13, 14) and even showed that the graft had completely eroded and replaced some areas of the aorta (15).
The patient in this video was a 49-year-old man who was first diagnosed with an aortic valve regurgitation with dilated ascending aorta at the age of 19. He remained under surveillance by a cardiologist, however he continued manual and heavy work. He was referred for his first operation when he was 39 years old. Perioperative transesophageal echocardiogram confirmed a severely incompetent aortic valve with a marginally enlarged left ventricle with good contractility. The ascending aorta was 48 mm with sinuses diameter of 45 mm. The aortic valve was tricuspid with fusion of the right and noncoronary cusps. There was some calcification on the tip of all leaflets and on each commissural level. The valve was excised and a 29 mm Mosaic bioprosthetic aortic valve was implanted. The dilated ascending aorta was wrapped with a 36 mm Dacron graft.
He remained well for following nine years after his first operation, then he developed symptoms of dizziness that generally lasted only for few seconds. His ECG confirmed heart block, therefore a permanent pacemaker was implanted that improved his dizziness. He underwent further investigations:
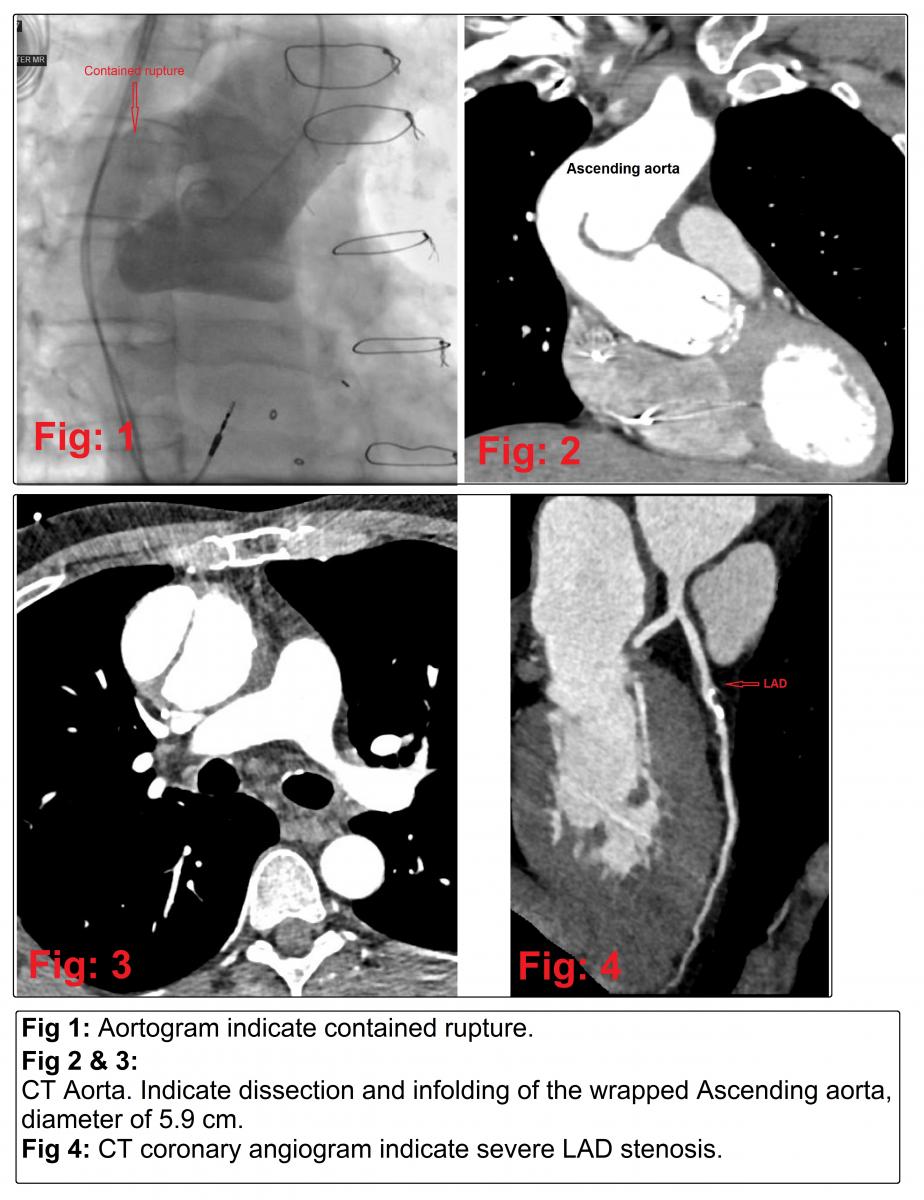
- Aortogram (Figure 1): indicate contained rupture.
- CT aorta (Figure 2): Dissection and infolding of the wrapped Ascending aorta. Proximal aortic arch measures about 42mm and mid arch 30 mm.
- CT aorta (Figure 3): Ascending aorta measures about 59mm at the level of the right pulmonary artery.
- CT-coronary angiogram (Figure 4): mid LAD plaques with severe stenosis. CT FFR was < 0.50 in the LAD beyond the stenosis. Other coronary arteries were normal.
He remained completely asymptomatic after getting his pacemaker. He was a current smoker for the last 30 years, using 30 cigarettes a day, otherwise there was no significant comorbidity. He was offered the redo operation, which he accepted. However, based on his clinical stability, the authors agreed to delay his operation, awaiting the resolution of the COVID-19 pandemic. Later, he was admitted one day before the operation as planned.
He underwent redo sternotomy, redo aortic valve replacement with Inspiris Resilia bioprosthetic aortic valve, size 27 (patient preference), and replacement of the ascending aorta with interposition Dacron tube graft 30 mm, plus one coronary artery bypass graft (saphenous vein grafted to LAD).
Operative Findings
The ascending aorta was severely dilated and pushed below the right hemi-sternum and firmly attached to the right atrium and superior vena cava. A contained rupture of wrapped ascending aorta is observed parallel to the native aorta contained by the pulmonary artery and the left atrial roof. Cumulative bypass time was 219 minutes, and cumulative cross clamp time was 165 minutes. His postoperative period was smooth and uneventful. He was discharged on the sixth postoperative day with very good recovery.
Operative Steps
The authors demonstrate, in this video, a technique to manage the contained rupture of wrapped ascending aorta by redo sternotomy, replacement of aortic valve, replacement of ascending aorta, and coronary artery bypass grafting.
Preparation Prior to Redo Sternotomy
The sternotomy was very high risk. it was not only a redo operation, but also a dilated ascending aorta with a contained rupture. The right femoral artery and vein were exposed. Also, the right axillary artery was exposed with a oblique incision, starting below the lateral and mid-third of the clavicle, and passed two nylon tapes around the axillary artery. A midline chest incision was created and divided the soft tissues up to the bone. They then passed two no 5 Ethibond sutures on the right side of the midline and another two no 5 Ethibond sutures on left side of the midline to pull and stabilize the sternum during redo sternotomy. They unntwisted the old sternal wires. They held the ends of the old sternal wires with the Spencer artery forceps but did not remove them. These old sternal wires indicate the limit of the posterior surface of the sternum during sternotomy.
Redo Sternotomy With the Oscillatory Saw
The authors used an oscillatory sternotomy saw to cut the partial thickness of the sternum. The sternal wires guided the posterior limit of the bone thickness. They held and pulled vertically upward the Ethibond sutures during the sternotomy. Then cut the sternum bit by bit using the oscillatory sternotomy saw to only a partial thickness. They used straight Mayo scissors to cut the remaining posterior periosteum and thick fibrous tissues. They removed the lower most sternal wire.
They then continued the same steps bit by bit as seen in the video. Start from the lower most part of the sternum and gradually progress towards the supra sternal notch. Therefore, first use the oscillatory saw to cut partial thickness of the sternum, then use straight Mayo scissors to cut the remaining posterior periosteum and thick fibrous tissues, and then remove the next lowest sternal wire. Constantly hold and pull vertically upward the Ethibond sutures.
Retrosternal Dissection
Use diathermy in the low setting to dissect the adhesions and release the heart from the chest wall. First, dissect the left side a few centimeters from the midline. Similarly, dissect the right side a few centimeters from the midline. Apply a retractor and open only a little, as opening wide may tear the heart
Findings
A severely dilated wrapped ascending aorta pushed below the right hemisternum and firmly attached to the right atrium and superior vena cava. A contained rupture of wrapped ascending aorta was observed parallel to the native aorta contained by the pulmonary artery and the left atrial roof.
Cardiopulmonary Bypass
A purse string suture was applied at the mid aortic arch (after the origin of the innominate artery) for aortic cannulation and to cannulate the aorta at the mid aortic arch. Pass a two stage venous cannula through the right atrium. Pass the retrograde cardioplegia cannula in the coronary sinus, through the right atrium. Then, commence cardiopulmonary bypass as routine for aortic valve surgery. Insert a purse-string suture in the right upper pulmonary vein and pass the LV vent. Further dissect and separate the heart from the pericardium and make a space at the aortopulmonary window for the aortic cross clamp. Apply the aortic cross clamp. Infuse antegrade cold blood cardioplegia and use ice slush topically.
Aortotomy and Inspection of Contained Rupture of Wrapped Aorta
Incise the aorta with a transverse incision. Findings: the true lumen of the aorta was on the right side, while the contained rupture of the aorta was on the left side. The aorta was extremely thin, severely atrophied, wrapped with the Dacron tube graft, and a defect/hole was in the wrapped aorta.
Dissection of the Aortic Root
Carefully dissect and separate the aortic root from the pulmonary artery. It was difficult to dissect the aorta from the surrounding adhesions and from the Dacron wrap as the native aorta was very atrophic. This dissection was very near to the left main stem, therefore use diathermy at low settings like 20. Also dissect and free from the right atrium. Give antegrade cardioplegia directly.
Excision of the Ascending Aorta
Excise the aorta 1 cm above the commissure level and 1 cm proximal to the aortic cross clamp.
Removal of Old Bioprosthetic Aortic Valve
First, place three 4-0 Teflon pledget prolene sutures at the sinotubular junction. Later, these sutures will pass through an external Teflon strip. Make a plane with the help of Watson Cheyne dissectors between the old valve annulus and the aorta. Please see the use of Watson Cheyne dissectors and artery forceps in the video, to make a plane between the old valve annulus and the aorta. Cut the old sutures with the number 11 knife. Remove the old pledgets and valve sutures bit by bit. Also use scissors to cut the sutures and strong tissues. Gently proceed little by little as the aortic tissues were fragile and may easily be torn. Finally, the old 29 mm Mosaic bioprosthetic aortic valve was removed.
Redo Aortic Valve Replacement With Inspiris Resilia Bioprosthetic Aortic Valve Size 27 (patient preference)
Place the interrupted valve sutures homogeneously, with 2-0 Ethibond with Teflon pledgets. Keep the Teflon pledgets in the infra-annulus position as the aortic valve will be implanted at the supra-annular position. Measure the valve annulus diameter with the valve sizers. In this patient, the Inspiris Resilia bioprosthetic aortic valve size 27 was selected. The valve suture was passed through the valve and the valve dropped down to the supra-annular position as it gave superior haemodynamic and left ventricular mass regression at the supra-annular position (16).
Coronary Artery Bypass Graft (Saphenous vein grafted to LAD)
Give antegrade cardioplegia directly. Check the vein. Finding a suitable site in the LAD can be difficult in redo cases. Open the LAD and anastomose the vein with the LAD by using 7-0 prolene sutures.
Replacement of the Ascending Aorta (with interposition Dacron tube graft of diameter of 30 mm)
Proximal Aorta Anastomosis
Prepare the proximal aorta edge. Take two Teflon strips. Place one strip at the outer surface and the other at the inner surface of the proximal aorta edge, circumferentially. Secure these strips with 4-0 prolene sutures. Afterward, measure the diameter of the outer surface of the aorta with the graft sizers. Here, the authors measure a 30 mm graft. They sutured the Dacron tube graft to the proximal aorta with a running suture of propylene 4-0. Start suturing from the posterior wall but finish anteriorly. Keep the initial posterior sutures loose, as a loop. Pass a Lahey forceps in between the loops, before pulling in these initial sutures, as seen in the video. This technique will help in placing the sutures parallel to each other. Check any leakage. Before proceed further, please look for any bleeding, especially behind the aorta, and secure hemostasis meticulously. Give cardioplegia through the Dacron tube graft and at this point, look carefully for any leakage through the aortic suture line. If you see any leak, mark it, and apply extra Teflon pledgets sutures at this stage. Apply Floseal at the suture line to seal the needle holes.
Distal Aortic Anastomosis
Prepare the distal aorta edge. Take two Teflon strips. Place one strip at the outer surface and the other at the inner surface of the distal aorta edge, circumferentially. Secure these strips with 4-0 proline sutures. Trim the distal Dacron tube graft to the appropriate length, as seen in the video. Suture the Dacron tube graft to the distal aorta with a running suture of propylene 4-0. Start suturing from the posterior wall but finish anteriorly. Keep the initial posterior sutures loose, as a loop. Pass a Lahey forceps in between the loops before pulling in these initial sutures. This technique will help in placing the sutures parallel to each other. Check any leakage. Apply extra Teflon pledgets sutures to any leak from the anastomosis.
Temporary atrio ventricular pacing wires were attached. De-air and wean off the cardiopulmonary bypass as routine and remove the venous pipe. See the final image of redo sternotomy, replacement of aortic valve, replacement of the ascending aorta, and CABG for the management of contained rupture of wrapped ascending aorta. Cumulative bypass time was 219 minutes. Cumulative cross clamp time was 165 minutes.
Tips & Pitfalls
- Attach external defibrillator pads before starting the redo operation.
- Prepare to go on cardiopulmonary bypass through the femoral vessels for any redo operation.
- Pass the retrograde cardioplegia cannula before commencing the cardiopulmonary bypass.
- Give antegrade or retrograde cardioplegia every 20-25 minutes.
- Check and recheck the aortic suture lines, specially posteriorly. Use extra interrupted sutures with/without a piece of Teflon for any suspicious leakage.
- De-airing: Do meticulous deairing in redo operations. The heart does not collapse completely in redo operation due to adhesions, therefore multiple air pockets remain inside.
References
- Ang KL, Raheel F, Bajaj A, Sosnowski A, Galiñanes M. Early impact of aortic wrapping on patients undergoing aortic valve replacement with mild to moderate ascending aorta dilatation. J Cardiothoracic Surg. 2010 Aug 6;5:58. PubMed PMID: 20691060; PubMed Central PMCID: PMC2922107.
- Tagarakis GI, Karangelis D, Baddour AJ, Daskalopoulos ME, Liouras VT, Papadopoulos D, Stamoulis K, Lampoura SS, Tsilimingas NB. An alternate solution for the treatment of ascending aortic aneurysms: the wrapping technique. J Cardiothoracic Surg. 2010 Nov 3;5:100. PubMed PMID: 21047398; PubMed Central PMCID: PMC2987920.
- Cohen O, Odim J, De la Zerda D, Ukatu C, Vyas R, Vyas N, Palatnik K, Laks H. Long-term experience of girdling the ascending aorta with Dacron mesh as definitive treatment for aneurysmal dilation. Ann Thorac Surg. 2007 Feb;83(2):S780-S784; discussion S785-S790.
- Tappainer E, Fiorani V, Nocchi A, Likaj E, Memishaj S, Zogno M. Safe wrapping of the borderline dilated ascending aorta during aortic valve replacement. J Cardiothoracic Surg. 2007 Feb 22;2:15. PubMed PMID: 17316443; PubMed Central PMCID: PMC1819379.
- Arsan S, Akgun S, Kurtoglu N, Yildirim T, Tekinsoy B. Reduction aortoplasty and external wrapping for moderately sized tubular ascending aortic aneurysm with concomitant operations. Ann Thorac Surg. 2004 Sep; 78(3):858-861.
- A. Olearchyk AS. Congenital bicuspid aortic valve and an aneurysm of the ascending aorta. J Card Surg. 2004 Sep-Oct; 19(5):462-463. PubMed PMID: 15383061
- Raheel FA, Hickey MS. Dacron Sleeve Around Ascending Aorta Without Excising the Aortic Tissues for Patients with Dilated Ascending Aorta Undergoing Aortic Valve Surgery; CTS net; 2012 Oct 15; Clinical Techniques » Cardiac Techniques.
- Plonek, T., Rylski, B., Dumanski, A. et al. Biomechanical analysis of wrapping of the moderately dilated ascending aorta. J Cardiothorac Surg 10, 106 (2015). https://doi.org/10.1186/s13019-015-0299-5
- Choi, Min Suk & Jeong, Dong & Lee, Hae & Sung, Kiick & Kim, Wook & Lee, Young & Park, Pyo Won. (2015). Aortic Wrapping for a Dilated Ascending Aorta in Bicuspid Aortic Stenosis. Circulation Journal. 79. 10.1253/circj.CJ-14-0933.
- https://www.ctsnet.org/article/dacron-sleeve-around-697-cm-ascending-aor...
- Neri E, Massetti M, Tanganelli P, et al. Is it only a mechanical matter? Histologic modifications of the aorta underlying external banding. J Thorac Cardiovasc Surg. 1999;118(6):1116-1118. doi:10.1016/S0022-5223(99)70111-X
- Dhillon JS, Randhawa GK, Straehley CJ, McNamara JJ. Late rupture after dacron wrapping of aortic aneurysms. Circulation. 1986;74(3 Pt 2):I11-I14.
- Bauer M, Grauhan O, Hetzer R. Dislocated wrap after previous reduction aortoplasty causes erosion of the ascending aorta. Ann Thorac Surg. 2003 Feb; 75(2):583-4.
- DOI: 10.1016/s0003-4975(02)04338-2
- Akgun S, Atalan N, Fazlio ğullari O, Kunt AT, Basaran C, Arsan S. Aortic root aneurysm after off-pump reduction aortoplasty. Ann Thorac Surg. 2010 Nov; 90(5):e69-70.
- Sang Hyun Kim, Ho Jin Kim, Joon Bum Kim, Sung-Ho Jung, Suk Jung Choo, Cheol Hyun Chung, Jae Won Lee, Supra-annular versus intra-annular prostheses in aortic valve replacement: impact on haemodynamics and clinical outcomes, Interactive CardioVascular and Thoracic Surgery, Volume 28, Issue 1, January 2019, Pages 58–64, https://doi.org/10.1093/icvts/ivy190
Acknowledgements
Thank you to Maaz A. Khan, and Zabreen Ahmed for editing and video narration.
Disclaimer
The information and views presented on CTSNet.org represent the views of the authors and contributors of the material and not of CTSNet. Please review our full disclaimer page here.



