ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Surgical Atrial Fibrillation - What We Must Do and What We Can Do
Monday, November 15, 2021
By Mark Gerdisch , Christian Shults, Armin Kiankhooy, Eric Okum, Marc La Meir, Patrick McCarthy, Laurie Barron, Gianluigi Bisleri, Niv Ad, Ralph J. Damiano Jr., M.D
PROGRAM OBJECTIVES
This activity is designed for cardiac surgeons in the United States. Upon completion of this course, participants will be able to learn the fundamentals of surgeons’ ability to very effectively treat atrial fibrillation and broadening our perspective on surgeons’ role in rhythm disorders.
RELEASE, REVIEW AND TERMINATION DATE
- Original release date: November 15, 2021
- Most recent review: November 15, 2021
- Termination date: November 15, 2022
DISCLOSURE POLICY
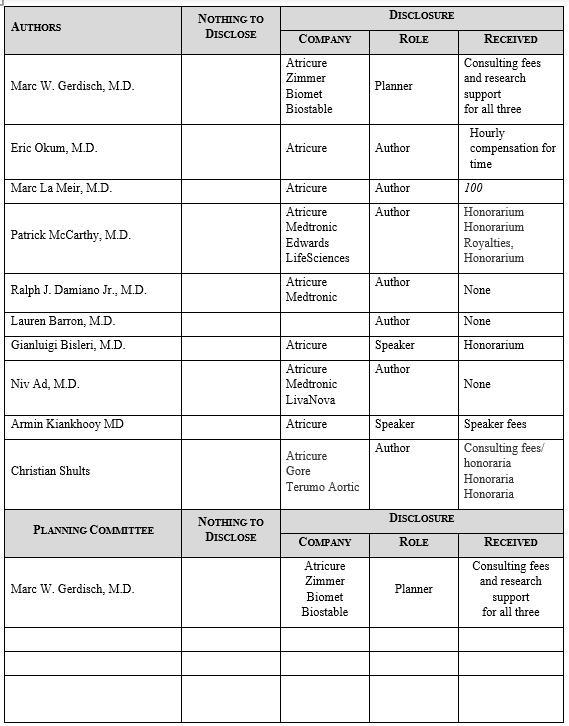
In accordance with the ACCME Accreditation Criteria, the American College of Surgeons must ensure that anyone in a position to control the content of the educational activity (planners and speakers/authors/discussants/moderators) has disclosed all financial relationships with any commercial interest (termed by the ACCME as “ineligible companies”, defined below) held in the last 24 months (see below for definitions). Please note that first authors were required to collect and submit disclosure information on behalf all other authors/contributors, if applicable.
The ACCME also requires that ACS manage any reported conflict and eliminate the potential for bias during the educational activity. Any conflicts noted below have been managed to our satisfaction. The disclosure information is intended to identify any commercial relationships and allow learners to form their own judgments. However, if you perceive a bias during the educational activity, please report it on the evaluation.
|
Ineligible Company: ACCME defines an “ineligible company” as any entity producing, marketing, re-selling, or distributing health care goods or services used on or consumed by patients. Providers of clinical services directly to patients are NOT included in this definition. |
|
Financial Relationships: Relationships in which the individual benefits by receiving a salary, royalty, intellectual property rights, consulting fee, honoraria, ownership interest (e.g., stocks, stock options or other ownership interest, excluding diversified mutual funds), or other financial benefit. Financial benefits are usually associated with roles such as employment, management position, independent contractor (including contracted research), consulting, speaking and teaching, membership on advisory committees or review panels, board membership, and other activities from which remuneration is received, or expected. ACCME considers relationships of the person involved in the CME activity to include financial relationships of a spouse or partner. |
|
Conflict of Interest: Circumstances create a conflict of interest when an individual has an opportunity to affect CME content about products or services of an ineligible company with which he/she has a financial relationship. |
Commercial Support Acknowledgement
CTSNet wishes to recognize and thank the following company for their monetary support: Atricure Inc.
Description of each video:
- Non Atriotomy Epicardial Ablation for AF by Eric Okum, MD
- This video demonstrates a novel non-atriotomy epicardial approach to the maze procedure with intraoperative testing.
- How to Perform a Hybrid Endocardial / Epicardial Mapping and Ablation for IST/POTS by Marc La Meir, MD
- This video will present a novel way to perform totally endoscopic, epicardial beating heart surgical ablation along with advanced epi-endocardial mapping in a hybrid setting.
- The Historical Perspective of the Cox Maze III by Patrick McCarthy, MD
- This video describes the development and evolution of the Cox Maze procedure is discussed by Patrick McCarthy, MD.
- Cox-Maze IV by Ralph J. Damiano Jr., MD, and Lauren Barron, MD
- This video demonstrates the Cox-Maze IV procedure for surgical ablation of atrial fibrillation via median sternotomy.
- Hybrid Ablation of Atrial Fibrillation With Advanced Epi-Endocardial Mapping by Gianluigi Bisleri, MD
- This video will present a novel way to perform totally endoscopic, epicardial beating heart surgical ablation along with advanced epi-endocardial mapping in a hybrid setting.
- Contemporary Strategies in Surgical Ablation for Atrial Fibrillation: Concomitant Ablation in Patients Without Mitral Valve Disease by Niv Ad, MD
- It has been shown that the Cox maze procedure is safe and effective with comparable outcomes when performed concomitant to mitral valve or non-mitral valve surgery.
- Shults Hybrid Therapy Convergent by Christian Shults
- The video demonstrates the technique for performing the FDA approved Convergent Procedure to treat persistent and long-standing persistent atrial fibrillation.
- Journey of an Afib Surgeon by Armin Kiankhooy MD
- The video provides insights into career opportunities and choices, and the evolution to advanced surgical treatment of atrial fibrillation.
Guest Editor Series Contributor Videos
- Non Atriotomy Epicardial Ablation for AF by Eric Okum, MD
- How to Perform a Hybrid Endocardial / Epicardial Mapping and Ablation for IST/POTS by Marc La Meir, MD
- The Historical Perspective of the Cox Maze III by Patrick McCarthy, MD
- Cox-Maze IV by Ralph J. Damiano Jr., MD, and Lauren Barron, MD
- Hybrid Ablation of Atrial Fibrillation With Advanced Epi-Endocardial Mapping by Gianluigi Bisleri, MD
- Contemporary Strategies in Surgical Ablation for Atrial Fibrillation: Concomitant Ablation in Patients Without Mitral Valve Disease by Niv Ad, MD
- Shults Hybrid Therapy Convergent by Christian Shults, MD
- Journey of an Afib Surgeon by Armin Kiankhooy, MD
To claim CME credits:
The American College of Surgeons designates this live activity for a maximum of 2 AMA PRA Category 1 Credits™. To receive a CME certificate, complete this survey form:
References
- Ad N, Holmes SD, Rongione AJ, Badhwar V, Wei L, Fornaresio LM, Massimiano PS. The long-term safety and efficacy of concomitant Cox maze procedures for atrial fibrillation in patients without mitral valve disease.J Thorac Cardiovasc Surg. 2019 Apr;157(4):1505-1514. doi: 10.1016/j.jtcvs.2018.09.131. Epub 2018 Nov 22.
- Badhwar V, Rankin JS, Damiano RJ Jr, Gillinov AM, Bakaeen FG, Edgerton JR, Philpott JM, McCarthy PM, Bolling SF, Roberts HG, Thourani VH, Suri RM, Shemin RJ, Firestone S, Ad N. The Society of Thoracic Surgeons 2017 Clinical Practice Guidelines for the Surgical Treatment of Atrial Fibrillation. Ann Thorac Surg. 2017 Jan;103(1):329-341. doi: 10.1016/j.athoracsur.2016.10.076. PMID: 28007240.
- Cox JL, Schuessler RB, D'Agostino HJ Jr, Stone CM, Chang BC, Cain ME, Corr PB, Boineau JP. The surgical treatment of atrial fibrillation. III. Development of a definitive surgical procedure. J Thorac Cardiovasc Surg. 1991 Apr;101(4):569-83.
- McCarthy PM, Castle LW, Maloney JD, Trohman RG, Simmons TW, White RD, Klein AL, Cosgrove DM. Initial experience with the Maze procedure for atrial fibrillation. J Thor Cardiovasc Surg 1993;105:1077-87.
- McCarthy PM, Cosgrove DM, Castle LW, White RD, Klein AL. Combined treatment of mitral regurgitation and atrial fibrillation with valvuloplasty and the Maze procedure. Am J Cardiol 1993;71:483-6.
- McCarthy PM, Gillinov AM, Castle L, Chung M, Cosgrove D. The Cox-Maze procedure: the Cleveland Clinic experience. Semin Thorac and Cardiovasc Surg 2000;12:25-9.
- McCarthy PM, Manjunath A, Kruse J, et al. Should paroxysmal atrial fibrillation be treated during cardiac surgery? J Thorac Cardiovasc Surg. 2013;146(4):810-823.
- Lee R, McCarthy PM, Wang EC, et al. Midterm survival in patients treated for atrial fibrillation: a propensity-matched comparison to patients without a history of atrial fibrillation. J Thorac Cardiovasc Surg. 2012;143(6):1341-1351; discussion 1350-1341.
- Musharbash FN, Schill MR, Sinn LA, et al. Performance of the Cox-maze IV procedure is associated with improved long-term survival in patients with atrial fibrillation undergoing cardiac surgery. J Thorac Cardiovasc Surg. 2018;155(1):159-170.
- Iribarne A, DiScipio AW, McCullough JN, et al. Surgical Atrial Fibrillation Ablation Improves Long-Term Survival: A Multicenter Analysis. Ann Thorac Surg. 2019;107(1):135-142.
- Cox JL, Malaisrie SC, Churyla A, Mehta C, Kruse J, Kislitsina ON, McCarthy PM. Cryosurgery for Atrial Fibrillation: Physiologic Basis for Creating Optimal Cryolesions.
- Gillinov AM, Gelijns AC, Parides MK, DeRose JJ Jr, Moskowitz AJ, Voisine P, Ailawadi G, Bouchard D, Smith PK, Mack MJ, Acker MA, Mullen JC, Rose EA, Chang HL, Puskas JD, Couderc JP, Gardner TJ, Varghese R, Horvath KA, Bolling SF, Michler RE, Geller NL, Ascheim DD, Miller MA, Bagiella E, Moquete EG, Williams P, Taddei-Peters WC, O'Gara PT, Blackstone EH, Argenziano M; CTSN Investigators. Surgical ablation of atrial fibrillation during mitral-valve surgery. N Engl J Med. 2015 Apr 9;372(15):1399-409. doi: 10.1056/NEJMoa1500528. Epub 2015 Mar 16. PMID: 25853744; PMCID: PMC4664179. Ann Thorac Surg 2020 Dec 3;S0003-4975(20)32039-7.
- Desai A, Thomas JD, Bonow RO, Kruse J, Andrei AC, Cox JL, McCarthy PM. Asymptomatic degenerative mitral regurgitation repair: Validating guidelines for early intervention. J Thorac Cardiovasc Surg. 2020 Nov 30:S0022-5223(20)33153-6. doi: 10.1016/j.jtcvs.2020.11.076. Epub ahead of print. PMID: 33419544.
- McCarthy PM, Herborn J, Kruse J, Liu M, Andrei AC, Thomas JD. A multiparameter algorithm to guide repair of degenerative mitral regurgitation. J Thorac Cardiovasc Surg. 2020 Oct 10:S0022-5223(20)32811-7. doi: 10.1016/j.jtcvs.2020.09.129. Epub ahead of print. PMID: 33168163.
- DeLurgio DB, Crossen KJ, Gill J, Blauth C, Oza SR, Magnano AR, Mostovych MA, Halkos ME, Tschopp DR, Kerendi F, Taigen TL, Shults CC, Shah MH, Rajendra AB, Osorio J, Silver JS, Hook BG, Gilligan DM, Calkins H. Hybrid Convergent Procedure for the Treatment of Persistent and Long-Standing Persistent Atrial Fibrillation: Results of CONVERGE Clinical Trial. Circ Arrhythm Electrophysiol. 2020 Dec;13(12):e009288. doi: 10.1161/CIRCEP.120.009288. Epub 2020 Nov 13. PMID: 33185144.
- Khiabani AJ, MacGregor RM, Manghelli JL, Ruaengsri C, Carter DI, Melby SJ, Schuessler RB, Damiano RJ Jr. Bipolar Radiofrequency Ablation on Explanted Human Hearts: How to Ensure Transmural Lesions. Ann Thorac Surg. 2020 Dec;110(6):1933-1939. doi: 10.1016/j.athoracsur.2020.04.079. Epub 2020 Jun 6. PMID: 32522634; PMCID: PMC7669627.
- Lancaster TS, Melby SJ, Damiano RJ Jr. Minimally invasive surgery for atrial fibrillation. Trends Cardiovasc Med. 2016 Apr;26(3):268-77. doi: 10.1016/j.tcm.2015.07.004. Epub 2015 Jul 20. PMID: 26296538.
- Khiabani AJ, MacGregor RM, Bakir NH, Manghelli JL, Sinn LA, Maniar HS, Moon MR, Schuessler RB, Melby SJ, Damiano RJ Jr. The long-term outcomes and durability of the Cox-Maze IV procedure for atrial fibrillation. J Thorac Cardiovasc Surg. 2020 May 5:S0022-5223(20)31065-5. doi: 10.1016/j.jtcvs.2020.04.100. Epub ahead of print. PMID: 32563577.
- Hybrid ablation for atrial fibrillation: current approaches and future directions. Bisleri G, Glover B. Curr Opin Cardiol. 2017 Jan;32(1):17-21
- Hybrid ablation for persistent atrial fibrillation: how to merge the best from both worlds. Bisleri G, Glover B. J Thorac Dis. 2017 Dec;9(12):4837-4839
- Preserved Left Atrial Epicardial Conduction in Regions of Endocardial "Isolation". Glover BM, Hong KL, Baranchuk A, Bakker D, Chacko S, Bisleri G. JACC Clin Electrophysiol. 2018 Apr;4(4):557-558
- Hybrid ablation for atrial fibrillation: the importance of achieving transmurality and lesion validation. Hassan SM, Hong K, Rosati F, Glover B, Redfearn D, Enriquez A, Bisleri G. Minerva Cardioangiol. 2019 Apr;67(2):115-120
- Ad N, Damiano RJ Jr, Badhwar V, Calkins H, La Meir M, Nitta T, Holmes SD, Weinstein AA, Gillinov M. Expert consensus guidelines: Examining surgical ablation for atrial fibrillation. J Thorac Cardiovasc Surg. 2017 Jun;153(6):1330–1354.
- Badhwar V, Rankin JS, Damiano RJ Jr, Gillinov AM, Bakaeen FG, Edgerton JR, Philpott JM, McCarthy PM, Bolling SF, Roberts HG, Thourani VH, Suri RM, Shemin RJ, Firestone S, Ad N. The Society of Thoracic Surgeons 2017 Clinical Practice Guidelines for the Surgical Treatment of Atrial Fibrillation. Ann Thorac Surg. 2017 Jan;103(1):329–334.
- Ad N, Suri RM, Gammie JS, Sheng S, O’Brien SM, Henry L. Surgical ablation of atrial fibrillation trends and outcomes in North America. J Thorac Cardiovasc Surg. 2012 Nov;144(5):1051–1060.
- McCarthy PM, Davidson CJ, Kruse J, Lerner DJ, Braid-Forbes MJ, McCrea MM, Elmouethi AM, Furguuson MA. Prevalence of atrial fibrillation before surgery and factorsassociated with concomitant ablation. J THorac and Cardiovasc Surg. 2020Jun;159(6):2245-2253.
- Ad N, Holmes SD, Rongione AJ, Badhwar V, Wei L, Fornaresio LM, Massimiano PS. The long-term safety and efficacy of concomitant Cox maze procedures for atrial fibrillation in patients without mitral valve disease. J Thorac Cardiovasc Surg. 2019 Apr;157(4):1505-1514.



