ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Excision of a Pulmonary Valve Papillary Fibroelastoma via Minimally Invasive Approach
Introduction
Minimally invasive surgery has become common for valve replacement and repair, as well as other forms of cardiac operations such as coronary artery bypass grafting and excision of cardiac tumors. Minimally invasive surgery technologies have developed over the past 20 years that have allowed for its increased application. Primary cardiac neoplasms are extremely rare, with an overall incidence of under 0.3% (1, 2). These pathologies mostly include three major types: myxomas, lipomas, and papillary fibroelastomas (PFE), with the relative frequencies of occurrence of 30%, 10%, and 8%, respectively (1). PFEs are benign tumors most frequently originating from the endocardium, comprising 70% to 90% of all valvular tumors, with the mean age of diagnosis at 60 years of age and occasional reports in children and teenagers (2, 3). In 95% of cases PFEs are localized to the left-sided valves with 44.5% of aortic valve and 36.4% of mitral valve involvement, while pulmonary and tricuspid valves are interchangeably cited as the least commonly involved (1, 2). Generali et al. report involvement of pulmonary valve in 8% of the papillary fibroelastoma cases, thus resulting in 0.00192% overall incidence of PV PFEs. According to Godwa et al., 43 PV PFE cases have been reported since 1856 (4), while other sources list 13 cases since 1931 (1). The authors present a novel, direct minimally invasive approach to the pulmonic valve via left anterior thoracotomy.
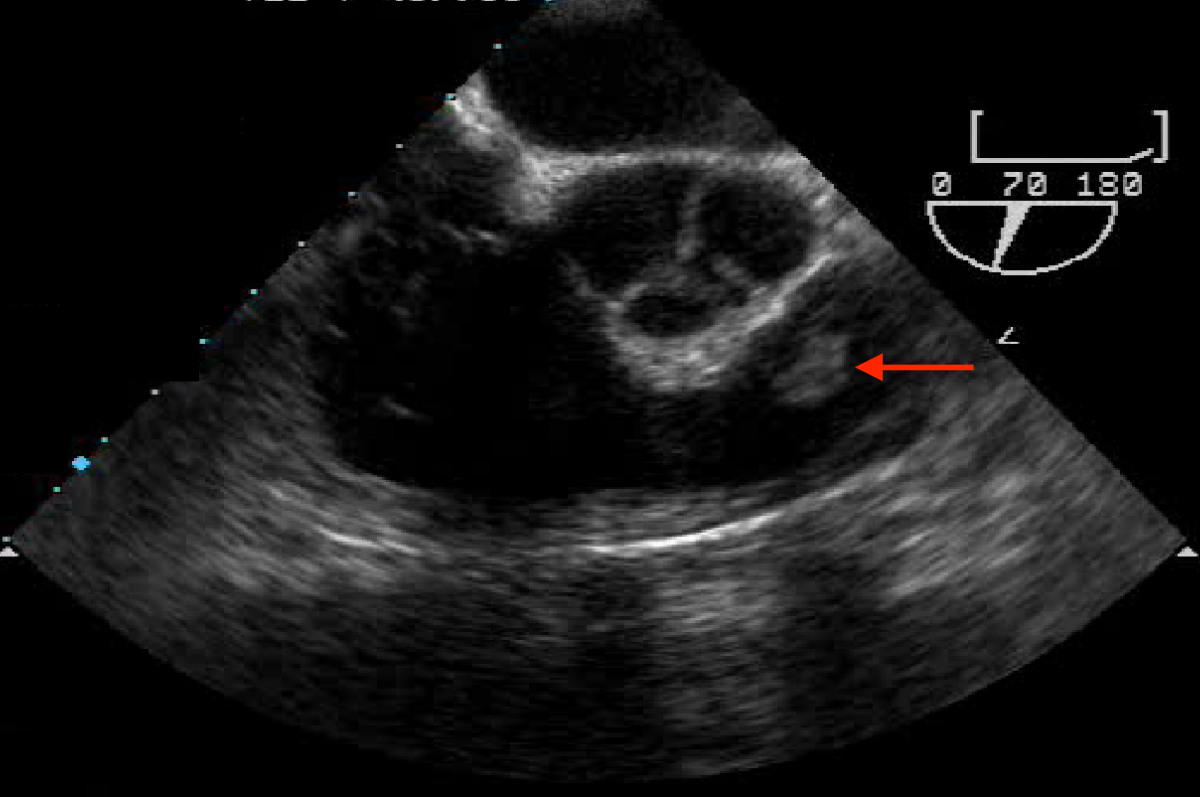
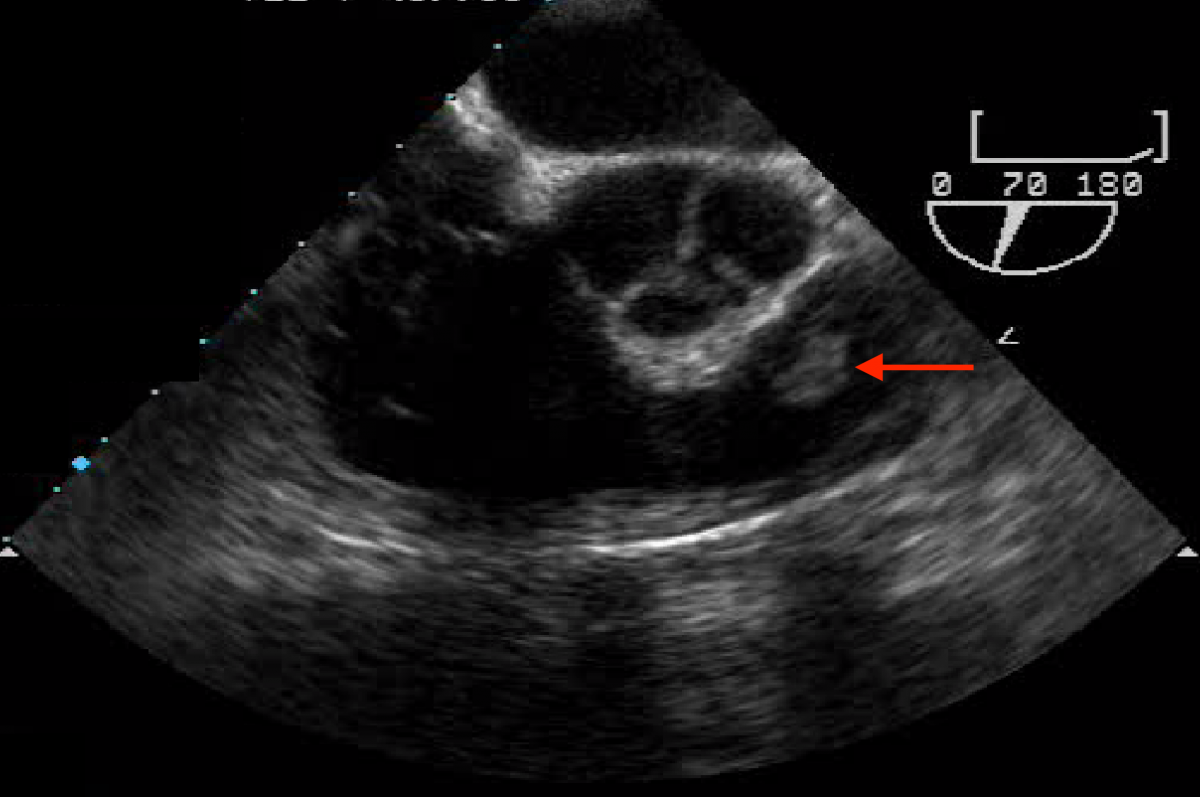
Figure 1: 1 cm tumor attached to the pulmonic valve.
Case Report/Description
A 56-year-old Caucasian male presented with exertional dyspnea, occasional palpitations, and night sweats. He underwent transthoracic echocardiography, which suggested a possible pulmonic valve tumor. A follow-up transesophageal echocardiography demonstrated a freely mobile, well circumscribed, nearly 1 cm tumor on the anterior leaflet of an otherwise structurally normal pulmonic valve (Figure 1). Contrast chest CT was remarkable for bilobulated tumor of the pulmonic valve consistent with a PFE (Figure 2).
Minimally invasive surgical excision was performed electively. The pulmonic valve was approached through a small left anterior thoracotomy incision overlying the second intercostal space. Standard peripheral cannulation for cardiopulmonary bypass was performed via the right femoral vessels. Upon initiating normothermic cardiopulmonary bypass, the pulmonary artery was opened revealing a 1.1 cm irregularly-shaped, tan-colored mass, which was attached to the posterior pulmonary leaflet. The tumor was completely excised from the leaflet without excising the leaflet tissue, and the pulmonary artery was closed. The patient made an uneventful recovery and was discharged on the fourth postoperative day in good condition. Pathology confirmed the diagnosis of PFE.
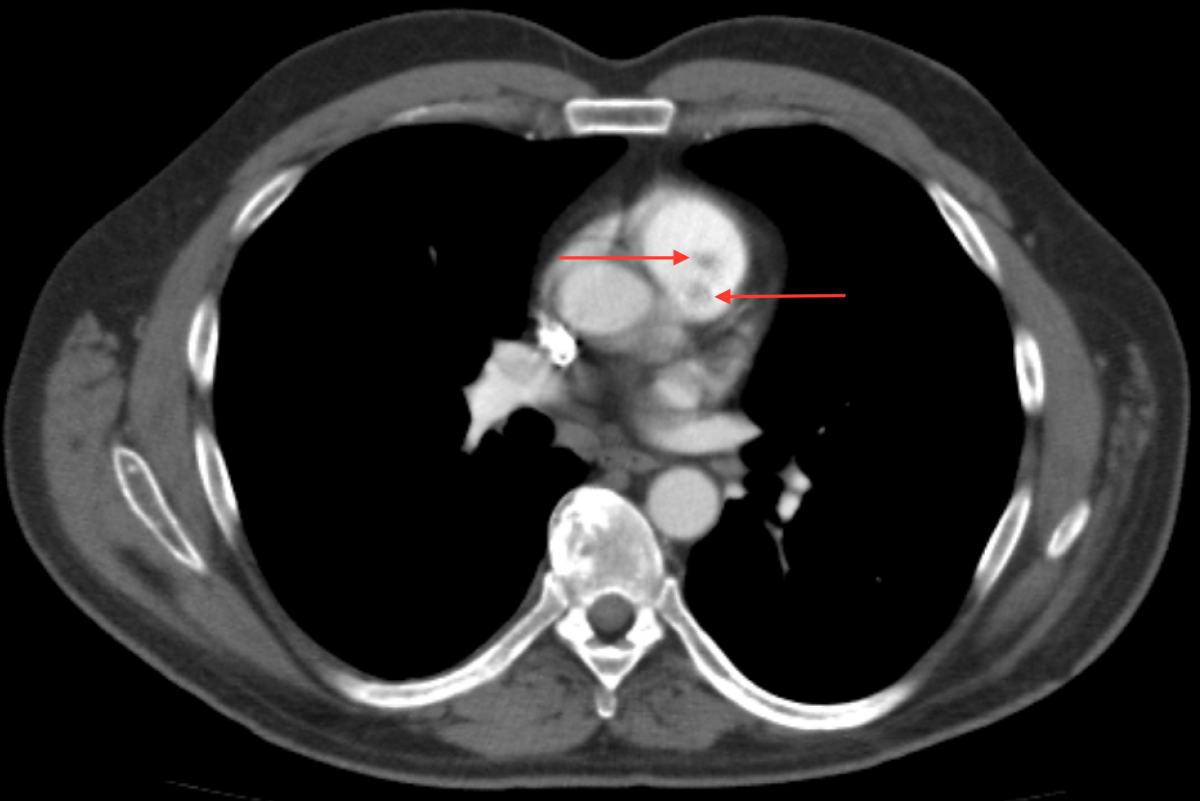
Figure 2: Two lobes of the pulmonic valve PFE
Comment
PFEs generally appear as solitary tumors, although occasional cases of multiple fibroelastomas have been reported (5, 6). PFEs usually appear as rounded, yellow, encapsulated, gelatinous masses, 15-20 mm in diameter, with multiple friable papillary projections on the surface (1, 2, 3, and 5). They are attached to the underlying endocardium with a short pedicle and are generally highly mobile (3).
PFEs have a tendency to be located on the atrial side of the atrioventricular valves, but have no preferential localization to either side, if semilunar valves are involved (3). While these tumors rarely cause valvular dysfunction, their localization and friable character can cause blockage of coronary ostial openings, turbulent flow, outflow obstruction, thrombus formation, and embolization, as well as dislodgment and embolization of fragments of the tumor itself (1, 3). In the case of left-sided tumors, this may clinically result in embolization to and obstruction of systemic circulation vessels in multiple organs. This most commonly leads to transient ischemic attacks, strokes, myocardial infarctions, as well as some retinal complications (1, 2, and 3). Gowda et al. documented a 50% PFE-related mortality rate, from either systemic embolization or outflow obstruction, in patients who did not undergo curative resection (4). While most of these patients had left-sided lesions, and it may not be possible to extrapolate data pertaining solely to right lesions, the potential complications of the right sided lesions cannot be ignored (4). Tumors located on the right-sided valves are typically asymptomatic, and before the use of echocardiography they were incidentally discovered at postmortem examinations (3). Tricuspid valve PFEs rarely lead to pulmonary embolism, and there are no reported cases of PV PFEs that have presented with symptoms (3, 7). However, due to their variable size and mobility, any valvular PFEs involve a potential risk of complications and are recommended to be surgically removed regardless of their size or location (1, 2, and 3). Due to the extremely low incidence and lack of information on pulmonic valve PFEs, there are no guidelines or protocols available regarding the management of these tumors and treatment options must be individualized depending on the specifics of the cases (1, 2, and 3). Before proceeding with surgical intervention, the tumor must be distinguished from other similar pathologies, such as other benign tumors or malignancies, thrombi, or vegetations (1, 3).
Once the diagnosis of PFEs has been established, surgical excision of the mass is a relatively simple procedure with an excellent prognosis (1). Unless the intraoperative appearance of the tumor suggests otherwise, fibroelastomas are simply removed without affecting the valve leaflets (5). Oakda et al. recommend inspecting the site of attachment and all cardiac chambers to ensure complete removal of the tumor (5).
The advent of minimally invasive techniques for aortic and mitral valve surgery has led to development of techniques and enabling technologies that have expanded the role of the minimally invasive approach. In this case tumor excision was easily achieved without the need for sternotomy or aortic cross-clamping. The patient was able to recover quickly and return to work soon after surgery.
References
- Generali T, Tessitore G, Mushtaq S, Alamanni F. Pulmonary valve papillary fibroelastoma: management of an unusual, tricky pathology. Interactive CardioVascular and Thoracic Surgery 16 [2013] 88–90
- Daccarett M, Burke P, Saba S. Incidental finding of a large pulmonary valve fibroelastoma: A case report. Eur J Echocardiography [2006] 7, 253e256
- Ibrahim M, Masters RG, Hynes M, Veinot JP, Davies RA. Papillary fibroelastoma of the pulmonary valve. Can J Cardiol Vol 22 No 6 May 1, 2006
- Gowda RM1, Khan IA, Nair CK, Mehta NJ, Vasavada BC, Sacchi TJ. Cardiac papillary fibroelastoma: a comprehensive analysis of 725 cases. Am Heart J. 2003 Sep;146[3]:404-10.
- Okada K, Sueda T, Orihashi K, Watari M, Matsuura Y. Cardiac Papillary Fibroelastoma on the Pulmonary Valve: A Rare Cardiac Tumor. Ann Thorac Surg 2001;71:1677–9.
- Sun JP, Asher CR, Yang XS et al. Clinical and Echocardiographic Characteristics of Papillary Fibroelastomas : A Retrospective and Prospective Study in 162 Patients. Circulation. 2001; 103: 2687-2693
- Howard RA, Aldea GS, Shapira OM, Kasznica JM, Davidoff R. Papillary fibroelastoma: increasing recognition of a surgical disease. Ann Thorac Surg. 1999 Nov;68[5]:1881-5.




{kind=link}