
ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
On Location: India

Affiliations: Division of Cardiovascular and Thoracic Surgery, University of Texas Southwestern (UTSW) Medical Center, Dallas, Texas, USA; Department of Cardiovascular and Thoracic Surgery, Amrita Institute of Medical Sciences (AIMS) Cochin, India; CEO and Director Frontier Lifeline Hospital, Chennai, India; Director, International Children’s Heart Fund
On Location: India
“If you observe from moment to moment how the mind gets caught in everlasting struggle-if you just observe the fact without trying to alter it, without trying to force upon the mind a certain state which you call peace-then you will find that the mind spontaneously ceases to struggle; and in that state it can learn enormously. Learning is then not merely the process of gathering information, but a discovery of the extraordinary riches that lie beyond the hope of the mind. "
Jiddhu Krishnamurti (1)
Introduction
On Location is an ongoing series designed to provide brief overviews of the evolution of cardiothoracic and vascular surgery (CTVS) programs and voluntary CTVS activities in developing countries. Surgeons with experience in the country create profiles wherein they provide relevant social and cultural background information, notes on the history of cardiothoracic vascular surgery (CTVS) in the country, and emerging trends in the field.
The On Location report highlights India, a country with major CTVS and related care needs. India bears 25% of the world’s burden of coronary artery disease (2). India remains an important emerging country with a growing economy. It is both a site for international help efforts and a case study in a society that has increased its CTVS importance and capability.
India is the seventh largest and second most populated country, with a population exceeding 1.34 billion (Table 1). Ten Indian states have populations greater than 60 million as of 2017, and the country has over 2000 ethnic groups with different lifestyles and distinct genetic ancestry, thus embodying the unique notion of “Nations within Nation” (6).
Table 1. India Statistics (2,3,4,5)
Population- 1,324,171,354 (2016)
Density- 382 people per.sq.km (2011)
Growth rate Increase- 1.19% (2016)
GDP Annual Growth Rate- averaged 6.16 percent from 1951 to 2018
Birth rate-19.3 births/1,000 population (2016)
Total Fertility Rate (TFR)-2.5 children born per woman (2016)
Death rate- 7.3 deaths/1,000 population (2016)
Mortality rate, under five (per 1000 live births) - 39.4 (2019)
Infant mortality rate- 32/1000 live births (2019)
Life expectancy at birth - 69.4 years (2019)
• Male- 68.2 years (2019)
• Female- 70.7 years (2019)
India’s practice of medicine has one of the world’s oldest recorded traditions. Dentistry and trepanation appeared as early as 7000 BC (7). The Indus valley civilization emphasized hygiene, sanitation, and medicinal plants. Theories and practices of ancient India remain consistent with modern western medicine. India has given birth to the science of Siddha, Ayurveda, Unani, and ancient medical texts such as Charaka Samhita, written by Charaka in the second century B.C, and Sushruta Samhita, one of the world’s earliest comprehensive surgical text by Sushruta approximately 2000 years ago (8).
India boasts a high degree of internal diversity wherein each region possesses distinct traditions, history, culture, and languages (Figures 1, 2). There lie differences between urban versus rural lifestyles in Indian society, and religion is important in molding one’s social identity. As per the 2001 census, India is 80.5% Hindu, 13.4% Muslim, 2.3% Christian, 1.9% Sikhs, 0.8% Buddhists, 0.4% Jain, and 0.6% other (9). Though religious conflicts occur, the country generally strives to maintain a secular ethos of inclusiveness, heterogeneity, and tolerance (Figure 3, 4).
Figure 1: Varanasi. River Ganges in the state of Uttar Pradesh (Photo courtesy of Dr. AT Pezzella)

Figure 2: Indian culture remains and flourishes (Photo courtesy of Dr. AT Pezzella)
Figure 3: “Krishna’s Butterball” - Balancing rock at Mahabalipuram in south India. (Photo courtesy of Dr. AT Pezzella)

Figure 4: Mahatma Gandhi (Photo courtesy of Dr. AT Pezzella)
India's continuing challenges are mitigating the maldistribution and imbalance between the poor vs. affluent, urban vs. rural populations, public help vs. curative care, public hospitals vs. private or charitable trust hospitals, and communicable diseases (CD) vs. non-communicable diseases (NCD). The WHO reports that deaths from coronary artery disease account for 18.25% of total deaths.
Economic divisions remain a notable feature of Indian society. The lifestyles of the wealthy and a slowly growing middle class appear in Indian media while many live with the realities of poverty. The World Bank defines extreme poverty as income < USD 1.90 a day (10). India has made rapid progress in the last two decades, with the extreme poverty rates dropping from 46% to 13.4%. Estimates show that 90 million individuals escaped extreme poverty from 2011 to 2015. India is still home to 176 million people living in poverty (10). The newer Multidimensional Poverty Index (MPI) ranks India at 129, with an estimated 27.9% of the population as penurious (11).
The Human Development Index (HDI) measures the effects of economics on quality of life. It considers the GDP, adult literacy, years of schooling, and a country's life expectancy. An HDI score over 0.80 is high, 0.50-0.79 medium, and less than 0.50 is low. India’s HDI human development index is 0.647, placing it in the lower end of the medium range (11). Life expectancy at birth is 69.4 years, about three years below the global average, and a healthy life expectancy is 57 years (11).
Indians feel a strong attachment to their region, culture, and traditions. India enjoys access to different technology and problem-solving approaches through globalization and continues to assimilate ideas from other regions of the world in areas that complement its storied traditions.
Ties between India and the United States continue to grow. India has been open to Western understandings, emphasized fluency in the English language, developed a solid domestic market, and maintained the world’s largest democratic government. In March 2020, during the US presidential visit to India, both countries agreed to designate their relationship as a “comprehensive global strategic partnership” and signed the Memorandum of Understanding, which addresses specific healthcare policies (12).
Cardiothoracic and Vascular Surgery (CTVS)
The growth and development of CTVS runs parallel with India’s rise in GDP (3, 13, and 14). The macro timeline of CTVS in India is outlined in Table 2 (15-27). The prevalence of coronary artery disease (CAD), rheumatic heart disease (RHD), congenital heart disease (CHD), and thoracic diseases, especially pulmonary Tuberculosis, is remarkably high. Addressing these diseases come with challenges that include late presentation, late referral, improper diagnosis, high out of pocket expenses, and disagreements over care pathways (i.e., medical, interventional, or surgical approaches). The age-adjusted mortality rate due to CAD has risen exponentially in the last two decades due to population growth, aging, and life style changes (28)
Table 2. Timeline of Cardiac surgery in India (15-27)
- 1946- Dr. KM Shah repaired an LV stab wound at King Edward Memorial (KEM) hospital Mumbai (earlier called Bombay).
- 1947- Dr. AV Baliga performed pericardial drainage of cardiac tamponade.
- 1948-1960- 1st CT surgery department established at Christian Medical College (CMC) in Vellore, by Dr. Reeve Hawkins Betts, a missionary surgeon from the USA. He performed PDA ligation (second in India) in 1950, first Potts-Smith shunt in 1951, first Classical Blalock-Taussig shunt in 1953 and first direct vision pulmonary valvotomy under inflow occlusion in 1953.
- 1948- Cardiological Society of India established
- 1949- Dr. Bomi R Billimoria performed the first PDA ligation at Masina Hospital in Byculla in Mumbai.
- 1952- Dr. PK Sen performed first successful closed digital mitral valvotomy at the K.E.M hospital, Mumbai
- 1953 - Dr. PK Sen performed the 1st coarctation repair’
- 1954- Thoracic Surgeons’ Association of India founded at Vellore
- 1956- Dr.PK Sen performs the first direct vision closure of ASD under surface induced Hypothermia and inflow occlusion.
- 1959- Dr. AK Basu performed first aortic valvotomy using inflow occlusion technique at Presidency General Hospital, Kolkata (previously Calcutta).
- 1960- 1st three candidates completed MS in Thoracic surgery from CMC Vellore under Madras University. They were Dr. N Gopinath, Dr.T. Thomas and Dr. G Allen.
- 1961 (16th February)- Dr.KN Dastur performs the first closure of Atrial Septal Defect using an Indian made Heart/Lung machine, in 19-year-old female patient at BYL Nair Hospital in Bombay
- 1961 (28th July) - Dr.N. Gopinath closed a VSD using a Heart/Lung machine at CMC Vellore.
- 1962 (13th April)- Dr. Radhakrishna Padhi and Dr. Fletcher did the intracardiac repair of congenital pulmonary stenosis under cardiopulmonary bypass in a 9 year old boy at Wanless mission hospital at Miraj.
- 1962- Dr N. Gopinath did first repair of TOF in CMC Vellore
- 1965- Dr GB Parulkar- left heart bypass for thoracic aortic aneurysm
- 1968- 16th February -Fifth heart transplant in the world, with short survival by Dr PK Sen.
- 1968- Dr Valiathan- Gott shunt for descending thoracic aneurysm
- 1974- 1st Department of Pediatric Cardiology established at CMC Hospital, Vellore
- 1975- Dr.K.M. Cherian performs the 1st CABG in India in Railway hospital in Perambur Madras (Now Chennai)
- 1978- Dr.K.M. Cherian performed CABG along with Aortic valve replacement
- June 1979- Dr.K.M. Cherian performs Trans-atrial repair of Tetralogy of Fallot and double outlet right ventricles in June.
- July 1979- Dr.K.M. Cherian performs the first successful Senning operation for transposition of great arteries. In the same year, he performs a successful Rastelli’s operation for transposition, VSD and pulmonary stenosis and used a fresh antibiotic sterilized homograft as RV to PA conduit.
- October 1980- Dr.K.M. Cherian performs the first successful arterial switch operation for transposition of great arteries with ventricular sepal defect with single coronary artery.
- 1982- Dr.K.M. Cherain performs the first anomalous left coronary artery from pulmonary artery (ALCAPA) repair in an 18-month-old child with severe mitral regurgitation.
- 1984- 1st Interventional PCI. Dr. SC Manchanda, AIIMS, New Delhi.
- 1980- Perfusion School-CMC Vellore
- 1990- The Indian Association of Cardiovascular and Thoracic surgeons (IACTS) was established and the publication of Indian Journal of Thoracic and Cardiovascular surgery (IJTCS) has commenced from 1982 onwards.
- 1990 Dr K.S. Iyer- first successful neonatal arterial switch operation
- 1992- Dr.K. S Iyer performs the first two-stage arterial switch operation for transposition with regressed left ventricle.
- 1993- Dr.K.S. Iyer performs the first double switch operation for congenitally corrected transposition and he subsequently performs the first aortic root transfer (Nikaidoh-Bex) for transposition with ventricular septal defect and pulmonary stenosis.
CTVS has progressed significantly in India. The Indian Journal of thoracic and cardiovascular surgery (IJTCVS) has addressed the evolution and challenges of CTVS in India by identifying plausible approaches to various concerns that include patient care, education, research, and administrative topics. In the 2019 presidential address, Dr. Yugal K Mishra made a vital quest for public-private partnerships, which will help improve the private sector's volume while decreasing the government costs of health care infrastructure. Thus, benefiting both parties (29).
Coronary Artery Disease (CAD)
Cross-sectional studies have shown a greater prevalence of CAD in India when compared to other industrialized nations (30, 31), with more than 32 million patients and makes up 25% of the world’s population with CAD. CAD is twice as prevalent in urban populations vs. rural population (7-10% vs. 3-5%). Lifestyle changes, stress, diet, chronic diseases (diabetes, hypertension, dyslipidemia), obesity and smoking, continue to contribute to this epidemic (30, 32). Ischemic heart disease and stroke are the predominant causes for >80% of CVD deaths (28.1% of the total mortality in India) in 2016 (33-36). There is a significant difference between CAD amongst Indians and the western population. CAD occurs in younger patients, is more diffuse, and has high case fatality rate.
The Global Burden of Disease study estimates that the age-standardized CVD death rate of 272 per 100 000 population in India is higher than the global average of 235 per 100 000 population (32, 33). In 2015 it was estimated that India had 2.1 million deaths due to cardiovascular causes, of which 0.9 million (68.4%) were aged 30-69 years. The death rate due to CAD increased from 10.4% to 13.1% in men and 4.8% to 6.5% in women from 2000-2015. This increase was higher in adults born in the 1970s and onwards, making it one of the world's youngest CAD cohorts. In addition, this young cohort also has multivessel involvement, diffuse disease, smaller vessels, poor ventricular function and higher Syntax scores (37, 38).
Cardiac Diagnostic Capability
There is wide gap of availability of cardiac diagnostic equipment between private and public healthcare facilities. Commonly available procedures such as stress ECHO, 64, 256, or 320 Multi-slice CT, Cardiac MRI, Coronary artery calcium screening, Coronary CT angiography, Holter monitoring, diagnostic angiography with catheterization, and nuclear medicine studies, often involve significant out of pocket expenses (39,40). Multi-slice CT with physiological assessment using Fractional Flow Reserve CT is also available to evaluate myocardial ischemia.
The SYNTAX III Revolution angiography fails to focus on clinical endpoints to decide the best treatment for complex CAD. Treatment decisions rely on clinical evaluation, and the combination of above tests.
Cardiac Interventional procedures, i.e., Percutaneous Coronary Intervention (PCI)
Coronary balloon angioplasty was developed in 1986, and coronary stents in 1991 (41-43). By 2008, more than 15 brands of drug-eluting stents (DES) were available in India (41).
Data on India's coronary interventional procedures are largely available through the National Intervention Council [NIC] and Industry. The NIC has developed a web-based system, which enables individuals and institutions to upload their data. There has been a steady 25-30 % in the number of annual interventions (43). The number of Cath-labs had risen from 251 in 2010 to 630 in 2015 and almost a 100% increase in interventions during the same period. In 2015, approximately 475,000 stents were used for 375,000 coronary interventions.
From an analysis of recent demographics, more septuagenarians are undergoing PCI (43). The number of female patients undergoing PCI has remained constant at 20–25 % of total interventions (43). Other available cardiology interventions include arrhythmic ablations, pacemaker and defibrillator device implantations, and heart valve or CHD interventions.
There is stronger demand for trained cardiologists and a greater need for a higher budget allocation to enhance training centers. Human resources remain a barrier to developing advanced facilities for interventional cardiology barring major cities. There are not enough organized training programs recognized by the Medical Council of India (MCI) or the National Board of Examinations (NBE).
Coronary Artery Surgery
Railway Hospital in Chennai, India, pioneered coronary surgery, where Dr. K.M. Cherian performed the first coronary artery bypass surgery (CABG) on a male patient on the 13th of June, 1975. Subsequently, he performed CABG on the first female patient on the 23rd April. 1976 (23). He also pioneered the use of left internal mammary grafts for CABG in September 1976, the use of intra-aortic balloon pump in 1977, and bilateral mammary arteries for CABG in 1981 (23). Today, CABG is one of the commonest cardiac operations in India, which has increased from 10,000 procedures annually in 1990’s to greater than 60,000 annually presently.
Given the increase in PCI, the patients referred for surgery are often late presenters with less attractive coronary anatomy often with diffuse triple vessel disease, small coronaries, poor ventricle function and poorly controlled diabetes with other comorbidities. Two studies have reported that there is high incidence of endarterectomy (14-16 %), in patients with diffuse disease undergoing CABG (44, 45).
Other available techniques in India include off-pump and minimally invasive coronary artery bypass grafting (OPCAB and MIDCAB), robotic surgery, and total endoscopic coronary artery bypass surgery (TECAB). OPCAB’s form 60% of CABG operations done in India mainly driven by economic reasons (46, 47).
In India, teams are seeking to refine their decision process by introducing ‘heart team’ (involving surgeons and cardiologists) concept, for decisions regarding lifestyle changes, medical management and interventional PCI vs. CABG. Yadava points out that the heart team should integrate patient selection by correcting it based on a physiological assessment of the stenosis (SYNTAX Score II or functional SYNTAX Score) along with the clinical profile, including comorbidities, and the refined SYNTAX Score III (38, 48-50). Unfortunately, cost and competition play a significant role in these decisions. Mishra (29) has stressed for development of criteria for the different care pathways, with the primary care physician actively involved, which would mitigate patient and family confusion regarding the integrated heart team approach.
Congenital Heart Disease
In India, an estimated 150,000-200,000 children are born with CHD each year, with an incidence of eight per 1,000 live births and form 10% of present infant mortality rate (51). Of these, nearly 70,000 to 100,000 suffer from critical CHD and require early intervention. The current medical infrastructure and human resource capacity are simply insufficient. If India were to follow the European association of cardiothoracic surgeons’ guidelines of having one congenital heart surgery center for every 4-6 million population, the country would need 215-325 dedicated pediatric cardiac surgical programs (52). Presently India has less than 25 exclusive pediatric cardiac centers, many of which are concentrated in only a few cities across India. Only 7-10% of neonates and infants in India with CHD receive timely surgery (51). An estimated 35% of cardiac operations are self-funded, 40% are government scheme funded and 20% through private donations and fundraising [53].
Care for CHD patients is challenging due to poor nutrition, poverty, delayed presentation, incorrect diagnosis, late referral, costs, access, available centers, and maldistribution of trained professionals such as pediatric cardiac surgeons, pediatric cardiologists, cardiac anesthetists, cardiac nurses etc. (54). In 2005, <5% of critical CHD patients underwent intervention. In addition, the increasingly critical and complex neonate CHD population puts a strain on the large backlog of cases needing surgery insofar as OR time and ICU beds are concerned. Presently, 25,000- 30,000 CHD operations are performed per year in India at 22 dedicated pediatric cardiac care centers (55-57).
Heart Valves
India has the world’s highest caseload for rheumatic heart disease (RHD), with a prevalence of valvar heart disease (VHD) at 1.5-2/1000 in all age groups (58-60). RHD prevalence represents 63.4 % of VHD in India (61). In 2015, the country had an estimated 13 million RHD cases resulting in 119,000 deaths (58-60).
India has a long experience with surgical and interventional treatment of RHD, including closed mitral valve commissurotomy, open mitral and aortic valve repairs, and valve replacements, and more recently minimally invasive, percutaneous, and robot approaches (62-64). India published one of the most extensive experiences of closed mitral valvotomy in the world (65). Percutaneous interventional mitral valve commissurotomies have been widely performed in India for rheumatic mitral stenosis (63). With the increase in lifespan, degenerative heart valve disease has also increased (64). India has extensive experience with its tilting disc mechanical valve prosthesis (TTK Chitra valve) (66) and indigenous production of homografts and xenografts (67, 68).
In 2019, Saksena et al. established a panel to create guidelines for the management of prosthetic heart valve patients with an emphasis on antithrombotic therapy (69). This is mainly in the RHD patients, given the challenges in lower income and rural populations. Yadava has cited this endeavor as a model for Indian cardiac surgeons to push forward for similar guidelines for other lesions (70).
Yadava addressed the progress of minimally invasive valve surgery (MICS) in India (71). He made the case that the younger generation of CTVS surgeons (below 40 years), be given preference for training in the MICS and advised the senior CTVS surgeons not to “compromise patient interests for reasons of ego, if they are not adequately trained.”
Thoracic Surgery
The Hindi word jugaad translates to “workaround,” a simple fix or innovation to a problem. This is so true for Indian surgeons dealing with thoracic diseases such as tuberculosis (TB), cancer, and trauma with varied resources (72-74). Yendamuri highlights the challenges of workforce shortage and affordability of operations (73).
In 2015, the incidence of TB was 1,740,435 cases with a prevalence of 320 per 100,000 population (75). The overall annual mortality was 510,000 (76-78). Out of this TB population, two to five percent need thoracic surgical intervention (78). However, there is a shortage of thoracic surgery practitioners. With the increasing incidence of drug-resistant tuberculosis in India and many patients with complications and sequelae of tuberculosis, there is a continuing challenge of addressing these patients' needs and the role of TB surgery (78, 79).
There are one million new cases of cancer annually in India. Lung cancer is the most common cancer among Indian men. Lung cancers makeup 6.9% of all new cancer cases and cause 9.3% of all cancer related deaths in both sexes. (80, 81). One to two million cancer deaths per year will occur by 2035, with 70,000 of those deaths secondary to lung cancer (82, 83).
Chest trauma, from motor vehicle accidents (MVA), is a significant problem in India (84-89). Common injuries include rib fractures, with over 60% requiring chest tube insertion (88). The mortality of MVA in India is 40% compared to 24% globally. An analysis of trauma deaths within 30 days of hospitalization in five urban university hospitals in India showed that overall proportion of preventable deaths was 58%, among the eligible deaths studied (87). Delayed hospital admission (1-2 hours) and few tertiary centers contribute to this.
Efforts have taken place to advance Indian health professionals’ training for handling trauma cases. The US-based ATLS course is available in India and organized by the Indian Society for Trauma and Acute Care (ISTAC) (89).
From one of the author's (ABM) experience, during training and conversation with residents from across India at Indian Association of Cardiovascular and Thoracic surgeons (IACTS) conference in 2020, it became evident that very few hospitals have dedicated general thoracic surgery departments. Often, cardiac surgeons with limited resources treat patients with thoracic diseases. Centers that train residents exclusively in Thoracic surgery are scarce. Another thoracic training track for residents is via thoracic surgical oncology teams. Without increased training positions in general thoracic surgery, there will be significant lacunae in trained personnel and expertise. Other factors for lack of good general thoracic programs include poorly trained and compensated dedicated thoracic surgery nursing staff, respiratory therapists, physical therapists, and biomedical engineers.
Nevertheless, recent advances in VATS and robotic surgery have opened a new era for training and practice. Many young surgeons revealed their desire to take up thoracic surgery and pursue fellowships (exclusively in VATS and robotics) overseas. An encouraging trend during the recent COVID 19 pandemic shows that the IACTS has initiated a master class program wherein virtual classes are being conducted, covering topics from general thoracic surgery. Going by the attendance of these webinars, there is a growing interest.
Perfusion training
Early surgeons have used indigenously built heart-lung machines which were often run by people, with various qualifications and varying training, including some assistant surgeons. The formal education and training in perfusion technology began at Christian Medical College, Vellore, in the 1980s with diploma courses in perfusion technology. In the year, 1983 the Indian society of Extra Corporeal Technology (ISECT) was started, followed by the creation of a program at King Edwards Memorial, Mumbai, in 1986 (90). In 1990, the IACTS, supported by Medtronic, Inc. USA, started a one-year course that included six months in basic medical sciences and six months of hands-on training. Subsequently, in 1992, Nizams Institute of Medical Sciences (NIMS) at Hyderabad introduced a two-year postgraduate diploma in clinical perfusion for the first time. Presently there are many bachelors, masters, and postgraduate courses available throughout the country (91).
Vascular Surgery
The CVTS surgeons in India were also practicing vascular surgery. However, slowly vascular surgery has evolved into a separate specialty. The first department of vascular surgery in India commenced in 1978, and in 1985, the first training course in peripheral vascular surgery (92). In 2008, there were only seven training centers for vascular surgery, with 12 trainees each year and 4,000 to 5,000 arterial reconstructions performed per year (92). As of 2016, there are 10 dedicated vascular surgery programs. Only about 70 full-time vascular surgeons are available for a population of one billion (92). There has been much hidden potential for vascular surgery in India, where there is continued progress as its demand increases (93).
The Vascular Society of India established the Indian Journal of Vascular and Endovascular Surgery in 1994 (94) marking the growth of this specialty. Vascular surgery is a fast growing specialty in India with growing interest in Aortic surgery, surgery for venous diseases, Endovascular surgery, hybrid surgery and state-of-the art vascular trauma management (93, 95, 96). Peripheral arteriolar disease (PAD) secondary to diabetes is increasing in India with ever increasing demand for vascular surgeons (97).
Cardiac and Lung Transplantation
India’s Dr. P.K. Sen was an early pioneer in heart transplantation and had the distinction of performing the fifth heart transplantation in the world in 1968. However, the patient had a short survival period (98). The first successful orthotropic heart transplant in India was carried out at AIIMS, New Delhi, in 1994 by Dr. P Venugopal and team (99). Dr.K.M. Cherian and his team performed the first Heart transplantation in India at a private hospital in 1995 (23). He later performed Heart-lung transplantation in 1998 and the first pediatric heart transplantation in 2009 (21, 23). Since then, numerous surgeons have performed cardiac transplants across India despite challenges such as donor organ scarcity, unsatisfactory organ support systems, infection risk, and prohibitive costs. Currently, there are over 60 centers performing heart transplants, which are primarily private hospitals and disproportionally concentrated to select cities in India.
Donor shortage in India is mainly due to lack of public awareness about altruistic value of organ donations and lack of knowledge about brain death. However, the donation scenario has improved in the last ten years, and now the challenge is dealing with the unutilized donor organs. Often, over 50% of donor organs are discarded for lack of suitable recipients, poor communication, poor donor management, transportation, lack of organized national registry, and costs. There is a need for coordinated organ allotment organizations in India. A heart transplant in India costs around USD 20,000- 30,000. Most of it is out of pocket expenses without insurance coverage. Risk of infections, continuation of immune suppressants and follow up are major challenges for heart transplant recipients in India.
Lung transplantation has had a slow growth in India since the first bilateral Sequential Lung Transplant, performed by Dr. K.M. Cherian and team in June 1997. Subsequently, Dr.N. Madhu Sankar and his team performed the first single lung transplant in 2011 (100). Presently fewer than ten centers perform Lung transplantation, as it is resource intense with involvement of pulmonologists, intensivists, anesthesiologists, and other medical professionals. It is also technically more challenging for surgeons who often need significant general thoracic training as well. The postoperative course is much more complicated, and the costs nearly double that of heart transplantation. However, in recent years, there has been a growing interest in them, and many centers are starting their lung transplant programs, especially in the post-Covid-19 era.
Anesthesia/ Critical Care
India has a well-developed Cardiac anesthesia (CA) program. Since its founding in 1997, the Indian Association of Cardiovascular and Thoracic Anesthesiologists (IACTA) has expanded to over 1,000 members (101,102). Borde et al. has outlined the importance of cooperation with perfusion in open-heart surgery (103).
Muralidhar effectively highlights the salient features of CA education, which includes cognitive knowledge base, psychomotor skills and affective material (104)
Critical care medicine advanced globally in the 1950s. One of India's first ICU and coronary care units was started in 1968 (105). The Indian Society of Critical Care Medicine (ISCCM) was established in 1993. Presently about 70,000 ICU, beds in India are available to the five million patients requiring ICU admission annually (106-108). The ISCCM, in 2010, published a guideline for the designing and functioning of Indian ICUs (107). Yeolekar, and Mehta in 2008, stressed the need to increase the ICU beds to 10% of total beds in all hospitals and 15-20% in the significant public and private tertiary care centers (108). The COVID pandemic has clearly highlighted the disparity in ICU care across India.
Summation of Clinical Aspects
An estimated six million Indians require cardiac surgery. Over 1,000 CTV surgeons perform cardiothoracic surgery in over 175 centers. Annual open-heart procedures exceed 140,000 (109). To put it into perspective, the US conducts 1,700 operations per million population. India performs a meager 130 operations per million population.
Cases of CAD are disproportionately higher in urban areas. Coronary artery operations account for 60% of all cardiac operations. The annual caseload has doubled since 1995 due to the increasing annual GDP, increase in procedural out-of-pocket payments, and the rising privately insured population.
India continues its struggle toward better medical infrastructure. Hishikar reminds Indian readers of Gandhi’s 1944 admonition to “burn Imperial Lancashire and Manchester cloths to relax British hold on our claim of independence” to emphasize the importance of domestic development (110).
India can manufacture indigenous medical equipment, devices, drugs, and disposables at reduced costs (figure 5). The medical device industry is growing exponentially (111,112). Indigenous products include the tilting-disc TTK Chitra Heart Valve, monitors, heart-lung bypass machine, electric sternal saw, surgical suture, surgical instruments, homografts, and xenografts (113). Recently, trans catheter valves are being developed locally (114). This being the case, health care costs are likely to increase as more medical products are being produced locally (115).
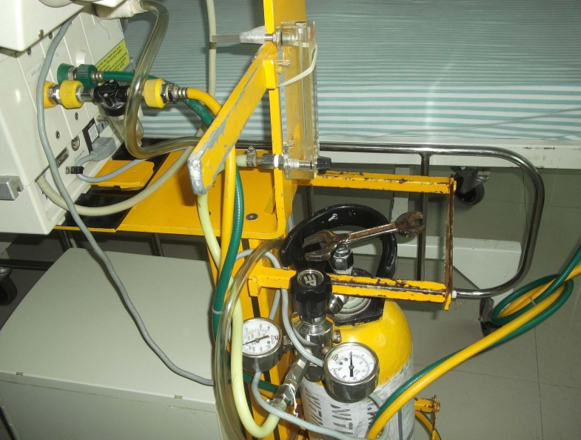
Figure 5: Homemade low cost Nitric Oxide device for CHD pulmonary hypertension (Photo courtesy of Dr AT Pezzella)
Foreign Contributions to India CT Surgery
The growth of CT surgery in India has accelerated through international assistance and has laid the foundation for a long-term goal of achieving a stable, sustainable and independent medical community. During and after British rule, individuals, missionaries, volunteers, corporate, NGOs, and surgical societies have advanced medical care and development.
Dr. Reeve H. Betts was a pioneer in CT care. Betts, from Boston, came to India as a medical missionary in 1948 and established the first accredited CVT residency program at Christian Medical College in Vellore (116). Other CT surgeons that visited India to teach surgical procedures include C Walton Lillehei, Charles Baily, Maghdi Yacoub, Paul Ebert, Christian Barnard, Denton Cooley, George Reul, Donald Ross, and many more (117).
Several early Indian CTV surgeons also pursued training abroad, in countries such as UK, USA, Canada, South Africa, Australia, and New Zealand. Many returned to India and pioneered CTVS surgery. Some of them include Dr. Solomon Victor, also referred as “a shining example of a Renaissance Man” (118), Dr. P. K. Sen (98), Dr. Kersi Dastur (19), Dr. N. Gopinath (22), Dr. Stanley John (22), Dr. Valiathan, Dr.K.M. Cherian (22,23), Dr.G.B. Parulkar, Dr. P. Venugopal, Dr.M.R. Girinath, Dr. I.M. Rao (22), Dr.K.S. Iyer (22), Dr. Naresh Trehan (119), Dr. Devi Shetty (120), and many others. Several senior Indian CTV surgeons like Dr. AS Kumar (121), Dr. KM Cherian (23), and Dr. Devendra Saksena (122) have been helping some Low and Mid income countries with their CVTS programs.
Some foreign associations include Children’s Heart Link, the Harvard Global Health Institute (123,124). The future role of voluntary foreign involvement includes individuals or teams coming to India for short-term training and specific new technology workshops.
CTV surgery education and training in India
“Tell me and I forget, teach me and I may remember. Involve me and I learn.”
Benjamin Franklin (125)
Background
Graduate medical education (GME) is a significant challenge in India (18), where early development of the field was hindered by colonialism. After inception in 1858, the General Medical Council (GMC) of Great Britain and the British Government intentionally worked to keep allopathic and health education in India on a lower profile than in Britain (126). The subsequent Medical Council of India (MCI), established in 1933, continued maintaining and advancing medical care standards and GME. The Bhore and Mudaliar Committees were established in 1943 and 1959 to manage the development and planning process of upgrading India's medical education
The MCI had control over certifying medical professionals in India for excellence and a responsibility to maintain a registry of certified professionals (127). Unfortunately, in 2017, MCI was involved in corruption prompting the government to replace the body and appoint five specialized doctors to monitor India's medical education system. Subsequently, in 2019 an ordinance was issued to replace MCI with National Medical Commission (NMC), and this process is still in transition.
As of 2016, the 412 medical schools in India admitted 53,000 students. About 40% (22,000) of these students complete a Bachelor of Medicine, Bachelor of Surgery (MBBS) degree annually (128). The traditional route involves many pursuing Postgraduate Degree programs such as Doctor of Medicine (MD), or Master of Surgery (MS). They then have the opportunity to pursue super specialization, which confers them a DM, or Master of Surgery (MCh, Latin: Magister Chirurgiae). In the alternative path includes postgraduate path via the Diplomate of National Board (DNB) route.
Current CTVS specialty
Indian medical students begin by earning their Bachelor of Medicine, Bachelor of Surgery (MBBS). Later they complete three years of general surgery residency with certification (MS/DNB) followed by three years of CTV surgery residency MCh (CVTS) or DNB (CT surgery). The respective universities certify MCh, whereas, the National Board of Examinations (NBE), certifies the DNB programs (129). Currently, the majority of Indian CTVS residency programs follow this 3+3-year model. A few programs offer a six-year integrated program straight out of medical school. All India Institute of Medical Sciences (AIIMS) is an autonomous public medical college of higher education declared by an act of parliament in 1956. They offer their own certification. In 2013, there were 50 CT surgery residency-training programs in India, with 100 seats available per year (130). The MCI recognizes both the MCh and the DNB training programs (130).
There are frequent debates regarding the balance of training times and the demands of patient care in these programs (MCh vs. DNB). Yadava reported that hospitals controlled by the MCI argued their programs offer better teaching and training compared to DNB programs which are largely in private hospitals (131). Valooran et al., in 2017, stressed the need for a modular concept that focused on competence, confidence, and performance (132).
In general, India’s education system may overvalue information mastery over adaptive problem-solving skills. In 2017, Shetty proposed a shift from information and knowledge to a competency ideology, which balances knowledge, skills and performance (133).
India’s CTVS training system suffers from imbalance and bias towards cardiac surgery. Only a few centers have well rounded programs with proper exposure to produce competent, mature, confident, and responsible trainees ready to perform. If CTVS were to attract quality candidates, the imbalance of clinical experience and providing more hands-on experience, needs to be addressed.
While many from India have been doing super fellowships abroad (North America, UK, Australia, and New Zealand) these positions are becoming scarce due to volatile immigration laws and more recently due to the pandemic. Could India fill this vacuum and become the next destination for surgical training? In a recent editorial, the author (a UK trainee) who spent significant time in India for training asks this critical question: “Could passage to India help with more training opportunities in the future?” (134). It may be the time for India to become self-reliant in CTVS training.
One Trainee’s Experience
One of the authors (ABM) recently finished his MCh (CTVS) training from AIIMS, New Delhi. AIIMS owns one of the most extensive CVTS University programs globally, where more than 4,000 open heart procedures are performed annually, comprising the entire spectrum of adult and pediatric heart surgery. The training spans three years, which also includes floor duties and ICU management of postoperative patients.
He was allowed into the Operating room (OR) and assisted cases from day one of his residency. The intensive training involved performing sternotomies and cannulations in the third month of training, closure of atrial septal defects by the sixth month, LIMA harvesting and proximal anastomosis by the first year, performing single valve cases independently by the second year, and by the final year being proficient in CABG and double valve cases. Final-year residents will also supervise first-year residents for ASD closures or cannulations. Such training allows for smooth transitioning into faculty wherein they will be capable of handling independent CABGs, valves, and some primary pediatric cases. This is a welcome transformation of a single training program with more hands on experience.
However, exposure to general thoracic surgery and training remained below par: the author’s one-month rotation in a thoracic center outside AIIMS was grossly inadequate. Other training gaps included the lack of exposure to intervention and wire skills, VATS and robotics, and Ventricular assist devices. Hence the sense of need for a super fellowship to fill in this gap.
The same author (ABM) further interviewed few MCh and DNB trainees during the IACTS national conference 2020 and gathered that training satisfaction varies across country programs. Common complaints included inadequate surgical exposure (pediatric cardiac surgery, general thoracic surgery), insufficient hands on experience and insufficient preparation for high stake decision-making thus necessitating continued mentored operative experience.
Another author (ATP) focused on CVTS training in India in 2008 (135). There has been some progress made in the training with more structure and some programs have even developed a comprehensive in-house manual for guidance (136, 137). There are calls for change in the curriculum from the current 3+3 program to a six year integrated curriculum (109) and to introduce “catheter wire skills” (138). Some programs have adopted the European Board of Cardiothoracic Surgery Syllabus in order to meet international requirements (139).
The need for quality individual mentorship looms large in India. In India, the mentor is likened to a guru who acts as a guide and teacher. Loop discusses the role of mentoring in CTV surgery (140). A CTV surgery career is divided into three phases: education, achievement, and giving back to the field. The mentor serves as a sponsor, advisor, and model. The mentor should have collegiality, knowledge, and reputation. Furthermore, the mentor should reflect competence, maturity, self-confidence, and a willingness to serve. Pasque proposed the revolutionary mentoring concept that emphasizes and focuses on the mentee(s) to set goals and establish milestones (141).
Sharma has articulated the ideal of the mentor or a ‘guru’ in Indian pediatric cardiac surgery training ‘gurukul’ or program (142). A guru is one who can inculcate in a trainee/ apprentice a sense of purposeful movements, concentration, accuracy and precision in small increments (142).
In 2018 Rao, gave tribute to his teachers and mentors and quoted Paul Soderberg on what a mentoring relationship ought to reflect: “More than mere teachers, mentors are often emancipators, freeing artists from poor technique, clouded vision and personal uncertainty” (143). Every cardiac surgeon in India is in search of a mentor of high caliber such as Wangensteen (144).
Pathways for Improving Training
Numerous Indian CTVS professionals seek training abroad. In 2018, Hinduja and Yadava noted that Indian post-residency training for essential surgical work was comparable to that provided abroad (145). However, international exposure was recommended for advanced cardiac surgical subspecialties that included minimally invasive cardiac procedures, robotic approaches, aortic and endovascular techniques, heart failure devices, and procedures.
Hands-on experience in CTVS training programs remains a challenge due to higher risk cases, technical difficulty, longer operative times, patient and referral issues, and faculty trainer attitudes. There remain issues with the oral and written examination and the certification process. The written and oral exams are somewhat objective, whereas the attending or faculty evaluation is subjective leading to wide variation in certification quality.
Simulation training, boot camp experience, corporate initiatives, and proctoring can supplement the above deficiencies (146). Meyerson et al. recommend a staged approach, which will offer a balance that leaves room for the differences in residence dexterity (147).
New portals for learning are being developed in India. Cardiac Surgeons in India (CSiI) is an independent nonprofit academic open learning management venture. It was designed for trainees (MCh or DNB) in Cardiovascular and Thoracic Surgery and the younger CTV surgeons in India and worldwide (148).
Generational Considerations
If India expands its CTVS community, it is vital to understand the generational factors that affect the CTVS professional community. Venute et al. looked at the worldwide differences in the CTVS community and their impact on education, training and biases (149). He divided them accordingly:
-Pre-Boomers (Silent) (born 1925–44; about 40 million people)
-Baby Boomers (born 1945–64; 79 million people; 55% of all active physicians)
-Generation X (born 1965–80; 61 million people; 30% of all active physicians)
-Generation Y (Millennial) (born 1981–99; 45 million people; 10% of all active physicians)
-Generation Z (born 2000–present)
There were obvious generational gap in thinking which can hamper progress. To learn about the goals and desires of the next generation, one of the authors (ATP) asked some CTVS residents and junior attending from around the world what three wishes they would have in terms of their lifestyle and career goals. The most common wishes were a complete residency experience; a job that provides growth, satisfaction, security, job incentives, decent salary, benefits; and quality time for personal interests and family needs. Dr. OP Yadava offers some sobering thoughts regarding CTVS and the medical profession itself, which run contrary to the above aspirations (150,151).
Research and Development (R/D)
There is a perception that India's medical research has not improved (152). There may be structural reasons for such and a lack of funding. The Indian Council of Medical Research (ICMR), with about 800 scientists working in 32 institutions, is the primary sponsor of R/D. The ICMR budget for 2017-18 was $232 million. By way of comparison, the US National Institute of Health budget was $32 billion, about 150 times higher (152).
In some CTVS programs in India, subsequent to clinical growth and residency program development, they are now focusing on R/D.
Many studies point to India's increased opportunities for epidemiological studies to prevent cardiovascular diseases and the role of translational research (153,154). Many investigators are mindful of the ethical implications of clinical and epidemiological research done in developing countries such as India. However, Indian programs may benefit from audits, review meetings, improved training and regulatory compliance (156). In 2004, the World Health Organization and the International Committee of Medical Journal Editors (ICMJE) published a joint editorial that promoted all clinical trials (157). The Indian Council of Medical Research (ICMR) in 2007 established the Clinical Trials Registry of India to encourage the registration of all clinical trials conducted in India (157).
The impact factor of an academic journal is a measure reflecting the yearly average number of citations to recent articles published in that journal (158). The official journal of IACTS is the Indian Journal of Thoracic and Cardiovascular Surgery (IJTCVS). It reports current clinical practices and developments in thoracic and cardiovascular surgery, including R/D results (159). The impact factor of this journal has been steadily increasing over the past three years.
The role of the IACTS, in concert with the IJTCVS, is crucial to the development of R/D in India. Unfortunately, the journal is not open access. The current editor of the IJTCVS, Dr. OP Yadava, has energized the journal with focused editorials and established standards for publication in the journal (160).
The other journal, which has greatly contributed to the growth of scientific work in congenital cardiac surgery, is the Annals of Pediatric Cardiology (161).
Laboratory research in fields such as stem cell research and tissue engineering has increased in India. One such is the Frontier Medeville model that offers several academic programs affiliated with other universities in India (162). They also collaborate with other international organizations that include the Korea Research Institute of Bioscience and Biotechnology, and the Singapore Cord Blood Bank. Cardiac surgeons in collaboration with the Indian Institute of Technology in Chennai have produced high-quality research in tissue engineering, stem cell research and development of indigenous xenografts. (163,164).
CTVS Database System Development
Another thing to consider is the CTVS community's ability to gather and teach from databases like that of the Society of Thoracic Surgeons (STS) or the European Society of thoracic Surgeons (ESTS). In India 1,000 cardiothoracic surgeons across 175 centers, perform approximately —70-80,000 cardiac operations/ year (179). However, there is no national Indian CTVS database system to report the procedures' quantity and quality. In the past IACTS failed in its attempts to create a national database. In 2018, Mangukia subsequently proposed that the IACTS take control of the database project and responsibility for data integrity and privacy (165). There are now renewed attempts to build a national database.
COVID 19 Pandemic
India imposed one of the earliest nationwide complete lockdowns. Such measures delayed the spread, but the country is now witnessing an escalation of cases (166). When writing this article (September 2020), India had the third highest count of cases (167). The pandemic has reinforced the need to strengthen public healthcare in India.
While on lockdown, the practice of cardiothoracic surgery was brought to a halt. To ensure that this did not negatively affect junior doctors' and resident trainees' minds, the leadership of the IACTS began organizing daily educational webinars via Zoom. Experienced faculty from all over the world took part in the program to ensure that education's quality is maintained to the highest standard. The series was named ‘MASTERCLASS’ and covered all aspects of adult and pediatric cardiac surgery, thoracic surgery, and transplantation. These webinars are curated by Drs.C. S Hiremath, V.V Bashi, K.S Iyer, A.Z Khan & Aditya N. Doddamane. Per Dr. Hiremath (168). This united the entire Indian cardiothoracic community as one, a “virtual family.” The program has been well received by professions from India and across the world (23 countries) (Figures 6-8).

Figure 6: Dr. Bashi, Dr. Hiremath, Dr. Iyer and Dr. Del Nido in a Master class.

Figure 7: Surgeons from IACTS with Prof.Anderson in a webinar on cardiac morphology

Figure 8: Figure 8. Prof. Nikaidoh with Drs. Hiremath, Dr. Iyer, Dr. Jaganath, Dr. Rao and Dr. Devagourou
Summary
"The roots below the earth claim no rewards for making the branches fruitful."
Rabindranath Tagore (169)
CTV surgery in India will continue to grow. Its surging demand has created a challenge to provide more centers. There is need for well-trained CTV surgeons, surgeons with wire skills, anesthesiologists, intensivists, perfusionists, cardiologists, nurses (Figure 9), and other staff. The increase in the quantity and quality of indigenous production of Indian biomedical equipment and disposables may well help offset the rising costs. With a collective effort, maldistribution can slowly dissipate. The increase in quantity, quality, and access to CT surgery will increase but require leadership and commitment. Affordability will remain a challenge, but Indian culture and beliefs will remain secure and relevant.

Figure 9: Educated, trained, and experienced Indian nurses are the backbone of Indian healthcare. (Photo courtesy of Dr. AT Pezzella)
Attracting CTVS residency candidates, along with helping them find a suitable and secure job on completion that balances incentive, satisfaction, and salary is necessary. In addition, time with family and personal needs or interests should be addressed. Team play, technology, and super specialization will supplement the new order. There remain room and support for the “up close and personal” doctor-patient relationship that encompasses both the public and private healthcare sectors. The future is bright with young surgeons taking on the mantle of CTV surgery in India (Figure 10).

Figure 10: Surgeons from various generations at IACTS 2020 (Photo courtesy of Dr. Kishor Joshi)
Acknowledgements:
Dr. Supreet Chopra, Dr. Manoj Durairaj for transplant data, Dr. Hiremath for IACTS master class data and pictures, Dr. Kishore Joshi for photograph, Mr. James, Ms. Nicole Goldberg, Joel Neil Murala and Dr. KS Iyer for editorial help.
References
- Krishnamurti J and Lutyens M. The Second Penguin Krishnamurti Reader. Harmondsworth [etc.]: Penguin Books.1970. Pg.161
- WHO India statistical profile. https://www.who.int/gho/countries/ind.pdf (Accessed 5/29/2020).
- India GDP Annual Growth Rate. https://tradingeconomics.com/india/gdp-growth-annual (Accessed 7/2/2020)
- World Bank’s Poverty Commission Releases Report on How to Better Measure and Monitor Global Poverty. https://www.worldbank.org/en/news/press-release/2016/10/18/world-banks-p... (Accessed 5/29/2020).
- Global Multidimensional Poverty Index. http://hdr.undp.org/en/countries/profiles/IND (Accessed 5/29/2020).
- Nations within a nation: variations in epidemiological transition across the states of India, 1990-2016 in the Global Burden of Disease Study. Lancet 2017; 390:2437-2460. DOI: https://doi.org/10.1016/S0140-6736(17)32804-0
- Boloor VA, Hosadurga R, Rao A, Jenifer H, Pratap S. Unconventional dentistry in India - an insight into the traditional methods. J Tradit Complement Med. 2014;4(3):153-158. doi:10.4103/2225-4110.130951 (Accessed 7/1/2020)
- Saini A. Physicians of ancient India. J Family Med Prim Care. 2016;5(2):254-258. doi:10.4103/2249-4863.192322
- Sharma OP. Change Comes Slowly for Religious Diversity in India – Population Reference Bureau [Internet]. Prb.org. 2020. Available from: https://www.prb.org/indiareligions/(Accessed 5/29/2020)
- World Bank’s Poverty Commission Releases Report on How to Better Measure and Monitor Global Poverty. https://www.worldbank.org/en/news/press-release/2016/10/18/world-banks-p... (Accessed 5/29/2020).
- Global Multidimensional Poverty Index. http://hdr.undp.org/en/countries/profiles/IND (Accessed 5/29/2020).
- 12. Trump’s visit may give healthcare shot in arm: http://timesofindia.indiatimes.com/articleshow/74250711.cms?utm_source=c... (Accessed 5/29/2020)
- Leirner AA. The health and wealth of nations- Coping with limited resources. Art Org.2006;30:493-497.
- Turina MI. Presidential address. European Association for Cardio-Thoracic Surgery: carrying the torch. Eur J Cardio-Thorac Surg 2002;22: 857–863.
- Hosain N. The early days of cardiac surgery in south Asia: The history and heritage. Ann Thorac Surg.2017;104:361-366. doi:10.1016/j.athoracsur.2017.01.039
- Das MK, Kumar S, Deb PK, Mishra S. History of Cardiology in India. Ind Heart J. 2015; 67(2):163–169. doi:10.1016/j.ihj.2015.04.004
- Parulkar GB, Gangal HT, Panday SR, Dhruva AJ, Sen PK. Left heart bypass for resectional surgery of thoracic aorta: An experimental study. Chest 1965;47:421-9. doi:10.1378/chest 47.4.421
- Valiathan MS, Weldon CS, Bender HW, Topaz SR, Gott VL. Resection of aneurysms of the descending thoracic aorta using a GBH-coated shunt bypass. J Surg Res. 1968;(8):197-205. Doi:10.1016/0022-4804(68)90086-3
- Kalke BR, Magotra RA. Tribute to Kersi Dastur, a pioneer in open-heart surgery in India. Ind J Thorac Cardiovasc Surg. 2010;26:228-232.
- Padmavati S. Development of cardiothoracic surgery in India. Ind J. Thorac Cardiovasc Surg. 2004;20:S50-S52.
- Ivatury RR. Developing congenital heart surgery in India. The travails and triumphs of a pioneer. Ann Ped Card.2018;11:174-180.
- Manohar SRK. Pioneers of congenital heart surgery in India: historical perspective. Indian J Thorac Cardiovasc Surg [Internet].2020. Available from https://doi.org/10.1007/s12055-020-00921-4 (Accessed 7/2/2020)
- Menon PM. Hand of God: A biography of Dr K M Cherian. Times Group Books. 2015. New Delhi, India
- Vaithianathan R, Panneerselvam S. Emerging alternative model for cardiothoracic surgery training in India. Med Educ Online 2013;18:1-4. 10.3402/meo.v18i0.20961
- Talwar S, Choudhary SK, Airan B, Juneja R, Kothari SS, Saxena A, et al. Reducing the costs of surgical correction of congenitally malformed hearts in developing countries. Cardiol Young. 2008;18(4):363–71. pmid:WOS:000258393300002.
- Choudhary SK, Srivastava S, Chander H, Sharma R, Venugopal P, Dogra TD, et al. Early experience with homograft valve banking. Asian Cardiovasc Thorac Ann.1997;5(3):137-40. Doi:10.1177/021849239700500303
- History IACTS [Internet]. Available from https://iacts.org/content/history (Accessed on 7/2/2020)
- Prabhakaran D, Singh K, Roth GA, Banerjee A, Pagidipati NJ, Huffman MD. Cardiovascular Diseases in India Compared With the United States. J Am Coll Cardiol. 2018;72(1):79‐95. doi:10.1016/j.jacc.2018.04.042
- Mishra, Y.K. Quest of affordable cardiac care with public-private partnership: a way forward to the future! Indian J Thorac Cardiovasc Surg. 2019;35:139–145. https://doi.org/10.1007/s12055-019-00810-5
- Krishnan MN. Coronary heart disease and risk factors in India - on the brink of an epidemic? Indian Heart J. 2012;64(4):364-7. Doi: 10.1016/j.ihj.2012.07.001.
- Joshi R, Jan S, Wu Y, MacMahon S. Global inequalities in access to cardiovascular health care: Our greatest challenge. J Am Coll Cardiol. 2008;52(23):1817–25.
- Prabhakaran D, Jeemon P, Roy A. Cardiovascular Diseases in India Current Epidemiology and Future Directions. Circulation 2016;133:1605–1620.
- Ke C, Gupta R, Xavier D, Prabhakaran D, Mathur P, Kalkonde YV, et al. Million Death Study Collaborators. Divergent trends in ischaemic heart disease and stroke mortality in India from 2000 to 2015: a nationally representative mortality study. Lancet Glob Health. 2018 ;6(8):e914-e923. Doi: 10.1016/S2214-109X(18)30242-0. PMID: 30012272; PMCID: PMC6942542
- Arokiasamy P. India’s escalating burden of non-communicable diseases. Lancet 2018;6:e1262-e1263. doi:10.1016/S2214-109X(18)30448-0
- Cardinal Features of CAD among Indians [Internet]. Available from http://www.cadiresearch.org/topic/asian-indian-heart-disease/asian-india...(Accessed 7/2/2020)
- Prabhakaran D, Jeemon P, Sharma M, Roth GA, Johnson C, Harikrishnan S, et al. The changing patterns of cardiovascular diseases and their risk factors in the states of India: the Global Burden of Disease Study 1990–2016. Lancet Glob Health 2018; 6: e1339–351.
- Modolo R, Collet C, Onuma Y, Serruys P. Syntax II and Syntax III trials: what is the take home message for surgeons? Ann Cardiothorac Surg 2018;7:470-482.
- Patel V, Chatterji S, Chisholm D, Ebrahim S, Gopalakrishna G, Mathers C, et al. Chronic diseases and injuries in India. The Lancet. 2011;377(9763):413-28.
- Non Invasive Cardiac Diagnostics -Safe Health Heart Centre [Internet]. 2020. Available from: http://safehealthindia.com/non-invasive-cardiac-diagnostics/(Accessed 6/30/2020)
- Outlook of India's Healthcare Industry [Internet], 2020. Available from https://www.surgerytoursindia.com/cardiac-diagnostic-services/ (accessed on 7/2/2020)
- Chaturvedi V, Talwar S, Airan B, Bhargava B. Interventional cardiology, and cardiac surgery in India. Heart 2008;94:268-274.
- Kaul U, Bhatia V. Perspective on coronary & cardiac surgeries in India. Indian J Med 2010;132:543-548.
- National Interventional Council, Cardiological Society India [Internet] Available from www.nicregistry.org (Accessed 7/2/2020)
- Cherian KM. The complexity of coronary artery disease in Indians- Issue with management. J Coron Heart Dis.2017;1:1.
- Padhy K, Narasimham SB, Murthy GS, Chaganti VR, Kumar PV, Rao MB, et al. Coronary endarterectomy for diffuse extensive coronary artery disease. Ind J Thorac Cardiovasc Surg. 2005;21(4):251-5.
- Saha KK. Off-pump coronary bypass grafting: the new gold standard! Ind J Thorac Cardiovasc Surg. 2018;34:3-5.
- Saha KK. Off-pump coronary artery bypass grafting in India. Ind Heart J. 2014;66:203-207.
- Yadava OP. CABG and PCI—just as we said it! Ind J Thorac Cardiovasc Surg. 2018;34:451–452.
- Deb S, Fremes S E. The SYNTAX battle in the war between stent and bypass. J Thorac Cardiovasc Surg 2016;152:1241-1242.
- Mack M, Baumgart H, Lytle B. Why surgery won the SYNTAX trial and why it matters. J Thorac Cardiovasc Surg 2016;152:1237-1240.
- Saxena A. Pediatric cardiac care in India: status and the way forward. Future Cardiol. 2018;14:1–4.
- Daenen W, Lacour-Gayet F, Aberg T, Comas JV, Daebritz SH, Di Donato R, et al. Optimal Structure of a Congenital Heart Surgery Department in Europe: by EACTS Congenital Heart Disease Committee. Euro J Card Thorac Surg.2003;24: 343-51. https://doi.org/10.1016/S1010-7940(03)00444-5
- Saxena A. Congenital Heart Disease in India: A Status Report. Ind Ped. 2018;55(12):1075-1082.
- Saxena A. Status of Pediatric Cardiac Care in Developing Countries. Children (Basel). 2019;6(2):34. doi: 10.3390/children6020034. PMID: 30823591; PMCID: PMC6406635.
- Kumar RK. Training pediatric heart surgeons for the future: A global challenge. Ann Pediatr Card 2015;8:99-102. Available from: http://www.annalspc.com/text.asp?2015/8/2/99/157020http://www.annalspc.c...(Accessed 7/2/2020)
- Rao S G. ‘Twists, travails & triumphs of pediatric and congenital heart surgery in India. Ind J Thorac Cardioivasc Surg. 2006;22:108–110.
- Saxena A. How to deliver the best: a call for congenital heart disease treatments in India. Future Cadiol 2014;10:359-366.
- Kumar RK, Tandon R. Rheumatic fever & rheumatic heart disease: The last 50 years. Ind J Med Res. 2013;137: 643–658.
- Shah B, Sharma M, Kumar R, Brahmadathan KN, Abraham VJ, Tandon R. Rheumatic heart disease: progress and challenges in India. Ind J Ped. 2013; 80 Suppl 1:S77-S86.
- Watkins DA, Johnson CO, Samantha M. Colquhoun SM. Global, Regional, and National Burden of Rheumatic Heart Disease 1990–2015. N Engl J Med 2017;377:713-722.
- Manjunath CN, Srinivas P, Ravindranath KS, Dhanalakshmi C. Incidence and patterns of valvular heart disease in a tertiary care high-volume cardiac center: A single center experience. Indian Heart J. 2014;66:320-326.
- Sampath Kumar A. Surgical options in rheumatic heart disease: an Indian surgeon's perspective [Internet, 2019 16th October]. Asian Cardiovasc Thorac Ann. 2019;218492319884797. doi: https://doi.org/10.1177/0218492319884797
- Sriram SN, Venkata BJ, Sadagopan T, Ramamurthy MT. Immediate, intermediate and long term clinical outcomes of percutaneous transvenous mitral commissurotomy. Int J Cardiol Heart Vasc. 2015;6:66-70. DOI: https://doi.org/10.1016/j.ijcha.2015.01.006
- Satsang DK. Sadasivan Oration- Search for the best heart valve- from replacement to repair. Ind J Thorac Cardiovasc Surg 2011;27:152-160.
- John S, Bashi VV, Jairaj PS, Muralidharan S, Ravikumar E, Rajarajeswari T, et al. Closed mitral valvotomy: early results and long-term follow-up of 3724 consecutive patients. Circulation. 1983 Nov;68(5):891–896.
- Sankarkumar R, Bhuvaneshwar GS, Magotra R, Muralidharan S, Rajan RS, Saha D, et al. Chitra heart valve: results of a multicenter clinical study. J Heart Valve Dis. 2001;10(5):619-627. https://www.ncbi.nlm.nih.gov/pubmed/11603602(Accessed 7/2/2020)
- Kumar S, Choudhary SK, Srivastava S, et al. Early Experience with Homograft Valve Banking Asian Cardiovasc Thorac Ann. 1997;5:137-140.
- Verghese S, Padmaja P, Sindhu B, Elizabeth SJ, Lesley N, Cherian KM. Homograft valve bank: our experience in valve banking. Indian Heart J. 2004;56(4):299-306.
- Saksena D, Mishra YK, Muralidharan S, Kanhere V, Srivastava P, Srivastava CP, et al. Follow-up and management of valvular heart disease patients with prosthetic valve: a clinical practice guideline for Indian scenario. Ind J Thorac Cardiovasc Surg. 2019; 35 (suppl 1):S3-S44. https://doi.org/10.1007/s12055-019-00789-z
- Yadava OP. First Indian practice guidelines in cardiac surgery .. Never too late! Ind J Thoracic Cardiovasc Surg 2019; 35: (Suppl 1):S1–S2
- Yadava OP. Minimally invasive cardiac surgery—a push to kaizen! Ind J Thorac Cardiovasc Surg 2018;34:(Suppl 2) S81–S8
- Yendamuri S. General thoracic surgery in India—the time is now. Ind J Thorac Cardiovasc Surg. 2018; 34:2–3. https://doi.org/10.1007/s12055-017-0629-4.
- Yendamuri S. Thoracic surgery in India: challenges and opportunities. J Thorac Dis. 2016 Aug;8(Suppl 8):S596-600. doi: 10.21037/jtd.2016.05.08. PMID: 27651933; PMCID: PMC5009067.
- Srikrisha SV. Progress in thoracic surgery. Indian J. Thorac Cardiovasc Surg 2009;25:96-101.
- Pai M, Correa N, Mistry N, Jha P. Reducing global tuberculosis deaths-time for India to step up. Lancet 2017;389 (10075):1174-1176. DOI: 10.1016/s0140-6736(17) s://www.thelancet.com/action/showPdf?pii=S0140-6736%2817%2930790-0 (Accessed 7/2/2020)
- India TB Report 2018 [Internet]. Available from https://tbcindia.gov.in/showfile.php?lid=3314 (Accessed 7/2/2020)
- Dewan RH. The challenge of pulmonary tuberculosis and the thoracic surgeon. Ind J. Thorac Cardiovasc Surg. 2006;22:111-115.
- TB statistics in India [Internet] – Available from https://tbfacts.org/tb-statistics-india/ (Accessed 7/1/2020)
- Shirodkar S, Anande L, Dalal A, Desai C, Corrêa G, Das M, et al. Surgical interventions for pulmonary tuberculosis in Mumbai, India: surgical outcomes and programmatic challenges. Public Health Action. 2016 Sep;6(3):193-198. doi: 10.5588/pha.16.0043. Epub 2016 21st September. PMID: 27695683; PMCID: PMC5034786.
- Behera D, Balamugesh T. Lung Cancer in India. Ind J Chest Dis. 2012;22:401-407.
- Mallath MK, Taylor DG, Badwe RA, Rath GK, Shanta V, Pramesh CS, et al. The growing burden of cancer in India: epidemiology and social context. Lancet Oncol.2014;15(6):e205-e212. doi:10.1016/S1470-2045(14)70115-9
- Malik PS, Raina V. Lung cancer: Prevalent trends & emerging concept. J Med Res. 2015;141:5–7.
- Noronha V, Pinninti R, Patil VM, Joshi A, Prabhash K. Lung cancer in the Indian subcontinent. South Asian J Cancer. 2016;5(3):95-103. doi:10.4103/2278-330X.187571
- Roy N, Veetil DK, Khajanchi MU, Kumar V, Solomon H, Kamble J, et al. Learning from 2523 trauma deaths in India opportunities to prevent in-hospital deaths. BMC Health Serv Res. 2017;17(1):142-150.
- Mohta M, P Kumar P, Mohta A, R Bhardwaj R, Tyagi A, Sethi AK. Experiences with chest trauma: Where do we stand today? Ind J Crit Care Med 2006;10:25-28.
- Narayanan R, Kumar S, Gupta A, Bansal VK, Sagar S, Singhal M, et al. An Analysis of Presentation, Pattern and Outcome of Chest Trauma Patients at an Urban Level 1 Trauma Center. Indian J Surg.2018;80(1):36-41. doi:10.1007/s12262-016-1554-2
- Manay P, Satoskar RR, Karthik V, Prajapati RP. Studying morbidity and predicting mortality in patients with blunt chest trauma using a novel clinical score. J Emerg Trauma Shock 2017;10:128-33.Available from: http://www.onlinejets.org/text.asp?2017/10/3/128/212497
- Narayanan R, Kumar S, Gupta A, Bansal VK, Sagar S, Singhal M, et al. An Analysis of Presentation, Pattern and Outcome of Chest Trauma Patients at an Urban Level 1 Trauma Center. Ind J Surg. 2018;80(1):36-41. doi: 10.1007/s12262-016-1554-2. Epub 2016 19th October. PMID: 29581683; PMCID: PMC5866799.
- Welcome to Advanced Trauma Life Support® (ATLS®) Course of American College of Surgeons - India Program, J. P. N. Apex Trauma Center, AIIMS, New Delhi [Internet]. Atls.in. 2020. Available from: http://www.atls.in/home.htm . (Accessed 7/2/2020)
- Talwar S. “The Development, Practices, Certification Process and Challenges of Cardiovascular Perfusion in India”. 2011, Charles C. Reed Memorial Lecture at the Annual Seminar of the American Academy of Cardiovascular Perfusion [Internet]. http://www.theaacp.com/wp-content/uploads/2014/08/Reed_Lecture_2011_Talw...(Accessed 5/15/2020)
- Indian Society of Extra Corporeal Technology [Internet]. Available from https://isect.org/history.php (Accessed 5/30/2020)
- Sekar N. Education in vascular surgery: Critical issues in India. J Vasc Surg 2008;48:76s-80s.DOI:https://doi.org/10.1016/j.jvs.2008.08.108
- Dabas AK, Dhillan R, Gambhir RPS. Journey of hybrid procedures in peripheral vascular diseases. J Vasc Surg. 2017;66(1):323-325. doi:10.1016/j.jvs.2017.01.039 (Accessed 7/1/2020)
- Indian Journal of Vascular and Endovascular Surgery [Internet]. Available from http://www.indjvascsurg.org/aboutus.asp (Accessed 7/2/2020)
- Verma H, Rai K, Vallabhaneni S R, Tripathi R. History of Aortic Surgery in India. Ind J Vasc Endovasc Surg 2015;2:105-11. Available from: http://www.indjvascsurg.org/text.asp?2015/2/3/105/166942(Accessed 1/13/2020)
- Sharma D, Goyal G, Singh A, Sisodia A, Devgarha S, Mathur RM. Management of Vascular Trauma: A Single Center Experience. Ind J Vasc Endovasc Surg 2014;1:3-7. Available from: http://www.indjvascsurg.org/text.asp?2014/1/1/3/142354 (Accessed 7/2/2020)
- Narayanan S, Boologapandian V. How to approach a patient with peripheral arterial disease. Ind J Vasc Endovasc Surg 2018;5:274-80. DOI: 10.4103/ijves.ijves_51_18
- Professor Prafulla Kumar Sen 1915~1982. Ind J Thorac Cardiovasc Surg. 1982;(1):92–94 https://doi.org/10.1007/BF02664159
- Venugopal P. The first successful heart transplant in India. Natl Med J India. 1994;7(5):213‐215.
- Elumalai RS, Somasundaram G, Vaidyanathan K, Venkatraman R, Nainar M, Rahulan V. Single lung transplantation in India: an initial experience. Ind J Chest Dis Allied Sci. 2013;55(2):101‐103.
- History of Cardiac Anesthesia in India [Internet]. Available from http://www.iacta.co.in/about.html (Accessed 7/2/2020)
- Tempe DK, Malik I. History of Cardiac Anesthesia in India. J Cardiothorac Vasc Anesth. 2018;32(5):2344-2355. doi:10.1053/j.jvca.2017.12.034
- Borde DP, Joshi SS, Chakravarthy M, Malik V, Karthekeyan RB, George A, et al. A survey of practices during cardiopulmonary bypass in India: An Indian association of cardiovascular and thoracic anesthesiologist endeavor. Ann Card Anaesth. 2019 ;22:56-66.
- Muralidhar K. Teaching cardiac anaesthesia. Ann Card Anaesth 2008;11:75-6
- Chowdhury D, Duggal AK. Intensive care unit models: Do you want them to be open or closed? A critical review. Neurol India 2017;65:39-45
- Jayaram R, Ramakrishnan N. Cost of intensive care in India. Ind J Crit Care Med. 2008;12:5561.
- ICU Planning and Designing in India – Guidelines 2010 Guidelines Committee ISCCM [Internet]. Available from https://isccm.org/pdf/Section1.pdf (Accessed 2/14/2019).
- Yeolekar ME, Mehta S. ICU care in India--status and challenges. J Assoc Physicians India. 2008;56:221-222.
- Valooran G, Nair S. A Career in Cardiothoracic Surgery: A Passionate Choice [Internet]. Available from https://www.ctsnet.org/article/career-cardiothoracic-surgery-passionate-.... (Accessed 7/2/2020)
- Hishikar A. Changing paradigms, changing mindsets. Ind J Thorac Cardiovasc Surg 2012;28:105-108.
- The medical device industry in India [Internet]. Available from https://www.investindia.gov.in/sector/medical-devices#:~:text=The%20medi.... (Accessed 7/2/2020)
- Shah AR, Goyal RK. Current status of the regulation for medical devices. Indian J Pharm Sci. 2008;70(6):695-700. doi: 10.4103/0250-474X.49085. PMID: 21369427; PMCID: PMC3040860. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3040860/?report=printable(Accessed 7/2/2020)
- Chitra heart valve [Internet]. Ttkhealthcare.com. 2020. Available from: http://www.ttkhealthcare.com/heart_valve.htm (Accessed 7/2/2020)
- Myval associated with no device-related mortality at one year [Internet]. Cardiovascular News. 2020. Available from:https://cardiovascularnews.com/india-designed-myval-associated-with-no-d...(Accessed 7/2/2020)
- Kumar RK. Technology and healthcare costs. Ann Pediatr Cardiol.2011;4(1):84-6. doi: 10.4103/0974-2069.79634. PMID: 21677816; PMCID: PMC3104544. (Accessed 7/2/2020)
- Reeve H. Betts Fellowship. Ind J Thorac Cardiovasc Surg.1982;1:98. https://doi.org/10.1007/BF02664161 (Assessed 7/2/2020)
- Naidu KV. 50 years of Cardiac Surgery in India. Indian J Thorac Cardioivasc Surg.1996;12:1-2.
- Rosenfeldt F. Solomon Victor: leading cardiac surgeon in India and long-time supporter of Heart, Lung and Circulation. Heart Lung Circ. 2007;16(2):69. doi:10.1016/j.hlc.2007.02.091
- Dr. Naresh Trehan [Internet]. Available from https://www.medanta.org/dr-naresh-trehan/ (accessed 2/15/2020)
- Shetty V. Podcast Episode: Giants of Cardiothoracic Surgery: An Interview with Devi Shetty [Internet]. Ctsnet.org. 2020. Available from: https://www.ctsnet.org/article/podcast-episode-giants-cardiothoracic-sur... (accessed 2/15/2020)
- A Sampath Kumar [Internet]. Available from https://www.ctsnet.org/home/asampathkumar (accessed on 7/1/2020)
- 2019 Surgical Humanitarianism Award: DevendraS.Saksena [Internet]. Available from https://www.facs.org/ogb/award-winners/humanitarian/saksena (accessed 7/1/2020)
- Children’s Heart Link Center of Excellence [Internet]. Available from https://childrensheartlink.org/where-we-work/(Accessed 7/1/2020)
- Harvard Global Health Institute [Internet]. Available from https://globalhealth.harvard.edu/. (Accessed 7/1/2020)
- Benjamin Franklin quote [Internet]. Available from https://www.birmingham.ac.uk/Documents/college-artslaw/studentexperience...
- Sahai A. Medical Education in India: Introspection, Challenges and Reforms – A vision. J Anat Soc Ind. 2016;65:167-174. https://doi.org/10.1016/j.jasi.2017.02.011
- The Medical Council of India [Internet]. Available from https://www.mciindia.org/CMS/ (Accessed 7/1/2020)
- Deswal BS, Singhal VS. Problems of medical education in India. Int J Community Med Public Health. 2016;3(7):1905-1909.
- Welcome To National Board Of Examination [Internet]. Natboard.edu.in. 2020. Available from https://natboard.edu.in/ (accessed on 7/29/20)
- Vaithianathan R, Panneerselvam S. Emerging alternative model for cardiothoracic surgery training in India. Med Educ Online. 2013;18:1-4. doi:10.3402/meo.v18i0.20961
- Yadava OP. NBE versus MCI—the slugfest. Ind J Thorac Cardiovasc Surg 2018;34:93–94.
- Valooran GJ, Sebastian R. Modular training in cardiothoracic residency—practical considerations to revive and streamline Indian training systems. Indian J Thorac Cardiovasc Surgery.2017;33:361–368.
- Shetty VS. Moving toward a competency based training ideology. Indian J Thorac Cardiovasc Surg 2017;33:280-283.
- Davies P. Could a passage to India be the way to get more surgical experience. Br Med J.2012;345:e6637. doi: https://doi.org/10.1136/bmj.e6637
- Pezzella T. Evolution of cardiothoracic surgery residency training programs in India. Indian J Thorac Cardiovasc Surg 2008;24:157-163.
- Guidelines for Competency Based Training Programme in DNB- Cardio Vascular and Thoracic Surgery 2011 [Internet]. Available from https://www.iacts.org/wp-content/uploads/2014/02/DNB-6-yr-course-CTVS-Gu... (Accessed 1/13/2020)
- Syllabus D M / M Ch at the AIIMS [Internet]. Available from https://www.aiims.edu/aiims/academic/aiims-syllabus/Syllabus%20-%20DM%20.... (Accessed 12/20/2019)
- Yadava O. Training in Cardiovascular Surgery: Thoughts of a Key Opinion Leader [Internet]. Ctsnet.org. 2020. Available from:https://www.ctsnet.org/article/training-cardiovascular-surgery-thoughts-... (assessed on 7/2/2020)
- European Board of Cardiothoracic Surgery Syllabus, April 2017[Internet]. Available from https://www.ebcts.org/wp-content/uploads/2017/09/EBCTS-Syllabus-Septembe... (Accessed 7/2/2020)
- Loop F. Mentoring (Developing the Academic Surgeon: A Symposium). J Thorac Cardiovasc Surg 2000;119: Suppl s45-s48.
- Pasque MK. Extreme mentoring in cardiothoracic surgery. J Thorac Cardiovasc Surg 2015;150:785-789.
- Sharma R. Making of a pediatric cardiac surgeon, in India. Ann Pediatr Cardiol 2008;1:50-53.
- Rao SG. The trainer, the Trainee, and the Trained. Indian J Thorac Cardioivasc Surg 2016;32:165-173.
- Gott VL. Lillehei, Lewis and Wangensteen: the right mix for giant achievements in cardiac surgery. Ann Thorac Surg. 2005;79(6):S2210-3.
- Hinduja M, Yadava OP. First nationwide survey on the experience of Indian cardiac surgeons about international fellowship programs. Indian J Thorac Cardioivasc Surg 2018;34:525–529.
- Trehan K, Kemp CD, Yang SC. Simulation in cardiothoracic surgical training: Where do we stand? J Thorac Cardiovasc Surg 2014;147:18-24.
- Meyerson SL, Sternbach, Zwischenberger JB, Bender EM. Resident autonomy in the operating room. Ann Thorac Surg.2017;104:1062-1068.
- Home Page: CSiI Open Learning Venture [Internet]. Cardiac Surgeons in India Open Learning Venture. 2020. Available from: http://www.csiiopenlearning.com/(Accessed 7/2/2020)
- Venuta F. Education motivation… inspiration of generation Y. The evolution of our species. Eur J CardiothoracSurg.2014;46:761-766.
- Yadava OP. Editorial- Wake Up Call. Indian J. Thorac Cardiovasc Surg2017;33:193-194.
- Yadava OP. Returning smiles to medicine. Indian J Thorac Cardiovasc Surg 2019; 35:1–2.
- The Sorry State of Medical Research in India [Internet]. Available from https://health.economictimes.indiatimes.com/news/industry/the-sorry-stat... (Accessed 7/2/2020)
- Krishnan A, Yadav K, Kaur M, Kumar R. Epidemiology to public health intervention for preventing cardiovascular diseases: The role of translational research. Indian J Med Res 2010;132: 643-65.
- Anand A, Rao M. Recipe for translational research in INDIA: MD-PhD or PhD-MD? Ann Neurosci. 2013;20:85.
- Glickman SW, McHutchison JG, Peterson ED, Cairns CB, Harrington RA, Califf RM, et al. Ethical and Scientific Implications of the Globalization of Clinical Research N Engl J Med. 2009 19th February;360(8):816-23. doi:10.1056/NEJMsb0803929
- Jadhav M, Bhatt A. Ethics in clinical research in India: A survey of clinical research professionals' perceptions. Perspect Clin Res. 2013;4(1):4-8. doi: 10.4103/2229-3485.106368. PMID: 23533971; PMCID: PMC3601702.
- WHO Clinical trials [Internet]. Available from https://www.who.int/bulletin/volumes/86/8/08-010808/en/ (Accessed 7/2/2020).
- Impact factor- Indian J of Thoracic and Cardiovasc Surgery [Internet]. Available from https://www.researchgate.net/journal/0970-9134_Indian_Journal_of_Thoraci... (Accessed 1/13/2020)
- Indian Journal of Thoracic and Cardiovascular Surgery [Internet]. Available from https://www.springer.com/journal/12055 (Accessed 7/2/2020)
- Yadava OP. Scientific misdemeanor- are we regulated enough. Indian J. Thorac Cardiovasc Surg 2017;33:287-288
- Annals of pediatric cardiology [Internet]. Available from http://www.annalspc.com/ (Accessed 8/12/2020)
- Frontier Mediville [Internet]. Available from http://frontiermediville.com/home.html (Accessed 7/2/2020)
- Balasundari R, Bishi DK, Mathapati S, Naser SB, Cherian KM, Guhathakurta S. Nanocoated Botanical Scaffold in Salvage for Human Tissue Regeneration. J Biomater Tissue Eng.2012;(2):330-335.
- Mathapati S, Bishi DK, Venugopal JR, Cherian KM, Guhathakurta S, Ramakrishna S, et al. Nanofibers coated on acellular tissue-engineered bovine pericardium supports differentiation of mesenchymal stem cells into endothelial cells for tissue engineering. Nanomedicine (Lond). 2014;9(5):623‐634. doi:10.2217/nnm.13.76
- Mangukia CV. Creating a systemic national database—are we ready. Indian J Thorac Cardiovasc Surgery 2018; 34:530.
- Ram VS, Babu GR, Prabhakaran D. COVID-19 pandemic in India: Is the curve now flat? Eur Heart J 2020;3874-3876 doi: https://doi.org/10.1093/eurheartj/ehaa493
- Corona virus resource center data from Johns Hopkins university. https://coronavirus.jhu.edu/map.html (accessed on 7/11/2020)
- Personal communication with Dr. Hiremath the secretary of IACTS who has spear headed the “Masterclass” initiative of IACTS in India. Vide email on 9th July 2020.
- "Rabindranath Tagore." AZQuotes.com. Wind and Fly LTD, 2020. 31st May 2020. https://www.azquotes.com/quote/414818(Accessed 7/2/2020)
Disclaimer
The information and views presented on CTSNet.org represent the views of the authors and contributors of the material and not of CTSNet. Please review our full disclaimer page here.



