ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Replacement of the Ascending Aorta With Aortic Root Remodeling Without Coronaries Reanastomosis
Raheel FA, Ahmed A, Hadjinikolaou L. Replacement of the Ascending Aorta With Aortic Root Remodeling Without Coronaries Reanastomosis. May 2019. doi:10.25373/ctsnet.8069369.
De Bakey and Cooley, in 1956, first replaced an ascending aneurysm with the aid of cardiopulmonary bypass. Since then, several methods evolved for the surgical repair of the aortic root and ascending aorta aneurysms. Bentall (2), in 1968, first used his technique when he noticed that it would not be possible to join the aortic wall above the coronaries to an aortic prosthesis. In 1976, Zubiate and Kay (3) closed the coronary ostia with sutures and used GSV to do an end-to-side anastomosis onto the corresponding coronary artery. In 1978, Cabrol (4) used a single 8 mm Dacron tube that functioned to supply the entire coronary circulation. In 1996, Yacoub introduced the valve-conserving technique for aortic root aneurysm or dissection (5) while Tirone David developed the technique of remodeling the aortic root and preservation of the native aortic valve (6).
The above techniques involve not only manipulations of the coronary ostia but also leaving some aortic wall around the coronary buttons. Pseudoaneurysm at the suture lines (7) and bilateral coronary ostial stenosis (8) are often seen with the classic Bentall procedures. False aneurysm formation and progression of aneurysmal disease are the predominant causes for late reoperations after aortic root or ascending aortic replacement (9). In one study, the sites of the aortic false aneurysm were either aortic suture or coronary ostium (10). In another study, reoperation for false aneurysm and the presence of coexisting coronary artery disease requiring bypass grafting were the only significant predictors of late mortality (11).
Is it always necessary to mobilize the coronaries and do four anastomoses during aortic root surgery—two for the aorta and two for the coronaries? Moreover, a growing elderly population with multiple comorbidities, technical challenges like restricted mobility of the coronary ostia, fragile tissues, as well as lack of experience preclude cardiac surgeons from doing aortic root surgery.
Leon introduced a simple technique of aortic root remodeling without handling of coronary ostia. The authors excised most of the aortic root wall except around the coronary ostia; most of the remaining aortic root wall is also reinforced by external Dacron. This ultimately remains very minimal unsupported aortic root, hence using only proximal and distal aortic anastomosis in this technique.
The authors also used a special technique for the posterior aortic wall anastomosis with five interrupted Ethibond® sutures and covered with a rectangular pericardial patch. This allows the proximal suture line to be placed close to the coronary arteries (12). The use of this technique in elderly and fragile patients avoids the risk of hidden leak and false aneurysm.
Patient Selection
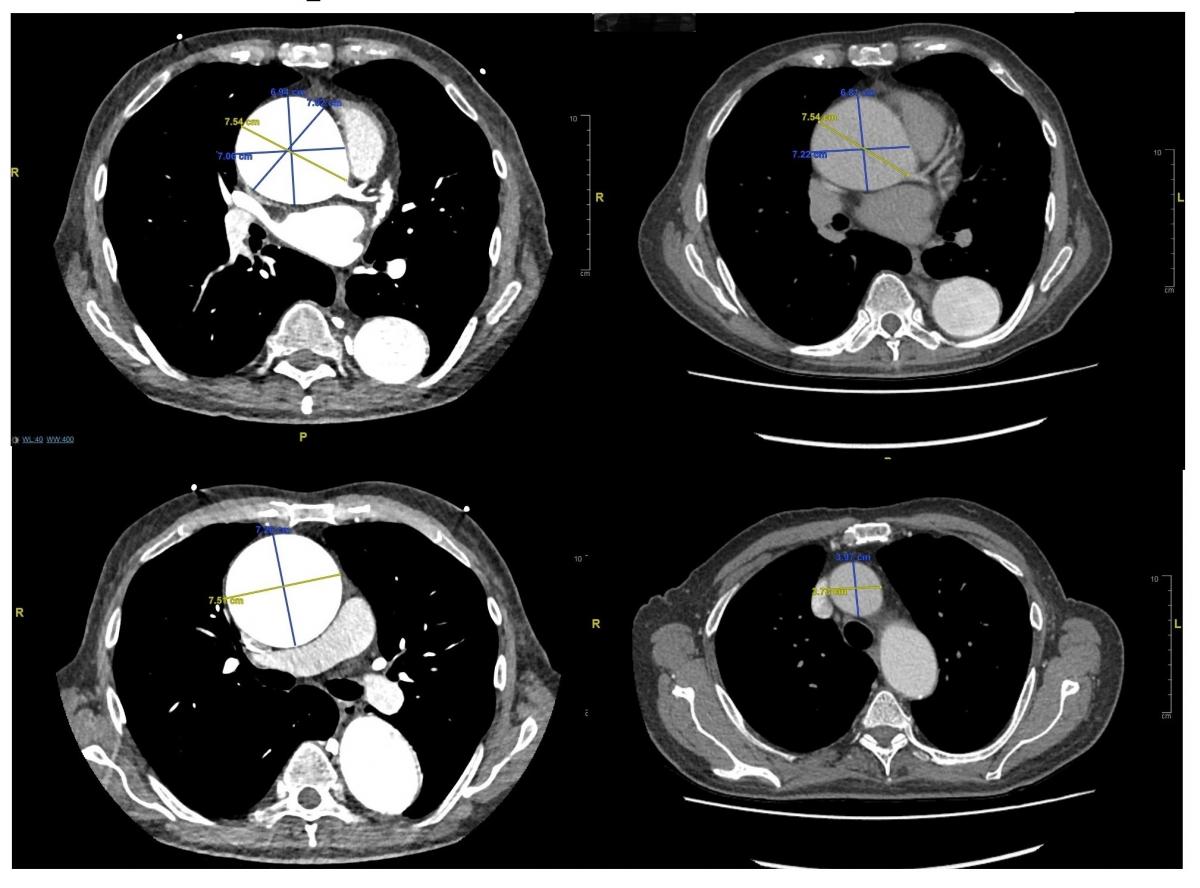
Figure 1. Preoperative CT scan.
The authors have been using this technique for several years. Patients were identified during preoperative work-up for aortic valve surgery or as incidental diagnosis. They selected those patients whose ascending aorta/root were aneurysmal and came under the European Society of Cardiology guidelines. All patients had preoperative computed tomography (CT) scan, echocardiogram, and immediate preoperative and postoperative transesophageal echocardiogram (TEE) that confirmed a wrinkle-free, smooth reduction of the aortic root diameter.
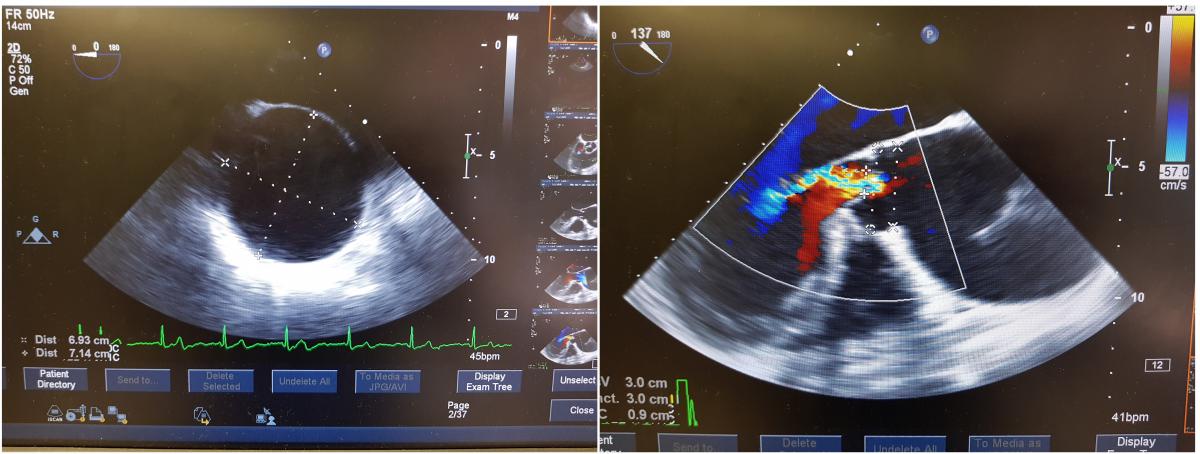
Figure 2. Preoperative TEE. (a) Short axis view and (b) and long axis view.
The patient in this video was a 73-year-old man who presented with acute abdomen; he later underwent appendectomy. During the abdominal investigation, he had a CT scan (Figure 1) and transthoracic echocardiogram.

Figure 3. Before and after ascending aorta replacement.
These tests showed that his ascending aorta and root were dilated up to 75 mm with severe aortic valve regurgitation, and his ejection fraction was 50%. His additive EuroSCORE was 11. Cumulative bypass time was 195 minutes, cumulative cross clamp-time was 142 minutes, and total circulatory arrest time was 32 minutes. He was admitted one day before the operation and was discharged on the seventh postoperative day with very good recovery.
Perioperative TEE is shown in Figure 2. Figure 3 depicts the operative field before and after the ascending aorta replacement.
Operative Steps (shown in video):
- Perform a routine median sternotomy and pericardiotomy.
- Extend the skin incision as T-shaped at the upper part of the midline skin incision. This will allow for accessing the brachiocephalic artery and left common carotid artery.
- Dissect the ascending aorta, as much as can easily be done, especially distally and in the aortopulmonary window.
- Pass the nylon tapes around the ascending aorta and brachiocephalic artery.
- Give heparin as usual.
- Select the aortic cannulation site at the distal aorta, 2 to 3 cm proximal to the level of brachiocephalic artery, at the reflection of the pericardium. Later, the cannulation site of the aorta will be excised with the aorta.
- Pass a two-stage venous cannula through the right atrium. Establish cardiopulmonary bypass as is done routinely for aortic valve surgery.
- Once again dissect and separate the ascending aorta from the surrounding tissues.
- Pass a nylon tape around the superior vena cava (SVC) and place a purse-string suture for the retrograde cerebral perfusion cannula.
- Make a purse-string suture in the right upper pulmonary vein and pass the left ventricular (LV) vent through the vein.
- Apply the aortic cross-clamp, incise and open the aorta, identify the coronary ostia, and infuse direct antegrade cardioplegia.
- Mark inside the aorta, 2 cm distal to the coronary ostia, to note the proximal aortic excision limit.
- Excise the aortic valve leaflets as routine. Excise the aorta 2 cm distal to the coronary ostia at the previously marked site.
- Place the aortic valve sutures with pledgeted Ethibond® 2-0 as routine, and repeat the cardioplegia administration through the coronary ostia.
- After repeating the cardioplegia, tie all valve sutures. Divide all of them except three, to be used as stay sutures.
- Start of aortic root remodeling.
- First step of aortic root remodeling:
- Pass three interrupted 4-0 Prolene® sutures through the aortic valve sewing ring then adjacent aorta and finally through the Teflon™ strips.
- Tie all three sutures. Do not cut the needles as the same sutures will be used for the next step of aortic root remodeling.
- Pass a single 4-0 Prolene suture through the aortic valve sewing ring at the junction between left and right coronary cusps. Then pass it through the adjacent aorta and then through the Teflon piece. Tie this suture. Again, don’t cut the needles as the same suture will be used for the next step of aortic root remodeling.
- Deep hypothermic circulatory arrest.
- Wait until the patient’s bladder temperature drops to 18-24oC.
- Repeat the administration of antegrade cardioplegia through the coronary ostia.
- Pass the retrograde cerebral perfusion cannula through the SVC.
- The authors used ‘manual inflate retrograde coronary perfusion cannula with integrated pressure monitor line’ as the cerebral perfusion cannula in this video.
- Snug down the nylon tape around the SVC.
- Stop the circulation, drain the blood through the venous line, and remove the aortic cannula. Attach the arterial line with the retrograde cerebral cannula.
- Remove the aortic cross-clamp.
- Excise the aorta, including the aortic cannulation site.
- Measure the diameter of the aorta with the clipper in order to select the appropriate Dacron tube graft with side arm. In the procedure shown in the video, the authors used a 26 mm diameter side-arm Dacron tube graft.
- Trim the appropriate length of the gelatine-impregnated Dacron side-arm tube graft.
Distal Aortic Anastomosis
- Perform the posterior aortic wall anastomosis, using a special technique for very secure hemostasis.
- First, place five interrupted 2-0 Ethibond sutures between the aorta and the Dacron tube graft
- Then, pass a thin Teflon strip between the threads and keep this strip at the outer surface of the aorta edge.
- Tie all five sutures individually and then divide them.
- Take a rectangle-shaped piece of bovine pericardium. Cover the five Ethibond suture knots with this piece of bovine pericardium.
- Use two 3-0 Prolene mattress sutures, as shown in the video.
- Tie these sutures; cut one end and keep the other end longer.
- Use the other long ends of these 3-0 Prolene to complete the aortic-Dacron anastomosis on both sides, keeping the Teflon strip at the outer surface of the aorta edge.
- Keep monitoring the cerebral oximeter during the circulatory arrest.
- Once the anastomosis is completed, dry the suture line with a swab, then apply the tissue glue over the suture line to seal the needle holes.
- Connect the arterial line via the connecter with the side arm of Dacron tube graft. Fill the aorta through retrograde transfusion via the SVC cannula. Remove the snugger from the SVC. Once the aorta and Dacron tube graft are filled with blood, apply the aortic cross-clamp over the Dacron tube graft.
- Re-establish cardiopulmonary bypass and remove the SVC retrograde cerebral perfusion cannula.
- Start rewarming. This is the benefit of doing the distal anastomosis first, as rewarming can begin at this stage.
- Trim the appropriate length of Dacron tube graft. First, mark on the tube graft. Keep the anterior length longer than the posterior length in order to achieve the natural curve of the aorta. Divide the graft with the scissors, as shown in the video.
- After re-establishment of cardiopulmonary bypass, repeat administration of antegrade cardioplegia through the coronary ostia.
Proximal Aortic Anastomosis, exactly same technique as the distal anastomosis.
- Perform the posterior aortic wall anastomosis.
- Place five interrupted 2-0 Ethibond sutures between the posterior wall of the aorta and the Dacron tube graft. When all five sutures have been placed, pass a thin Teflon strip between the threads and keep this strip at the outer surface of the aorta edge. Tie all five sutures individually and then divide them.
- Take a rectangle-shaped piece of bovine pericardium. Cover the five Ethibond suture knots with this piece of bovine pericardium.
- Use two 3-0 Prolene mattress sutures, as shown in the video.
- Tie these sutures; cut one end and keep the other end longer.
- Use the other ends to complete the anastomosis, keeping the Teflon strip at the outer surface of the aorta edge.
- Once the anastomosis is completed, dry the suture line with a swab, then apply the tissue glue over the suture line to seal the needle holes.
- Now start de-airing. First, fill the heart then use a size 14 IV cannula to puncture the Dacron tube graft as seen in the video. Once air bubbles have stopped, remove the aortic cross-clamp.
Second Step of Aortic Root Remodeling
- Three sutures were left with the needles attached at the noncoronary sinus.
- Please watch the video to see how the authors do the reinforcement of the remaining aortic root using external Dacron.
- Cut a rectangular shaped piece of Dacron.
- In the previous remodeling step, three interrupted 4-0 Prolene sutures were used and those sutures were passed through the aortic valve sewing ring, then the adjacent aorta, and finally through the Teflon strips. These sutures were left uncut in the previous step. Now pass these three Prolene sutures through the one long edge of the piece of Dacron and tie these sutures.
- Trim the piece of Dacron, as shown in the video.
- Use another three new 4-0 Prolene pledgeted sutures and attach the other long edge of this rectangular piece of Dacron with the adjacent Dacron ascending aorta.
- Tie these three sutures and divide the remaining length.
- Now this rectangular-shaped Dacron piece has been fixed on both long sides and provides extra support to this part of the aortic root.
- One suture has been left with the needle at the commissure between left and right leaflet.
- Cut a square-shaped piece of Dacron. In a previous step a single 4-0 Prolene sutures was passed through the aortic valve sewing ring at the junction between left and right aortic cusps, then through the adjacent aorta, and finally through the Teflon strips. That suture was left uncut in the previous step.
- Now, pass this Prolene suture, through the one long edge of this piece of Dacron and tie it. Use a new 4-0 Prolene pledgeted suture to attach the other long edge of this piece of Dacron to the adjacent Dacron ascending aorta.
- Now this square-shaped Dacron piece has been fixed on both long sides and provides extra support to this part of aortic root.
- Come off of cardiopulmonary bypass routinely. Please reference the final image of replacement of the ascending aorta with aortic root remodeling without coronary reanastomosis.
Tips & Pitfalls
- Convert the midline incision to a T-shaped incision after the sternotomy, at the level of left brachiocephalic vein. This will allow the good exposure of the aortic arch branches.
- Pass nylon tape around the left brachiocephalic vein and dissect to free this vein from the surrounding soft tissues. This will further expose the aortic arch and branches.
- The aortic cannulation site should be excised with the aorta.
- Retrograde cerebral perfusion flow should be between 400 and 800 ml per minute. Keep central venous pressure between 20 and 40 mm Hg.
- Continuously monitor the cerebral oximeter and titer the retrograde cerebral perfusion to keep the saturation of both sides, right and left, above 50%.
- Check and recheck the aortic suture lines. Use extra interrupted sutures if any leakage more than needle holes is observed.
- Do the distal aortic anastomosis first, and start gentle rewarming after completion of the distal anastomosis and re-establishment of cardiopulmonary bypass. This will save the total bypass time.
References
- Cooley DA, De Bakey ME. Resection of entire ascending aorta in fusiform aneurysm using cardiac bypass. J Am Med Assoc. 1956;162(12):1158-1159.
- Bentall H, De Bono A. A technique for complete replacement of the ascending aorta. Thorax. 1968;23(4):338-339.
- Zubiate P, Kay JH. Surgical treatment of aneurysm of the ascending aorta with aortic insufficiency and marked displacement of the coronary ostia. J Thorac Cardiovasc Surg. 1976;71(3):415-421.
- Cabrol C, Gandjbakhch I, Cham B. [Aneurysms of the ascending aorta; total replacement with reimplantation of the coronary arteries (author's transl)]. Nouv Presse Med. 1978;7(5):363-365.
- Yacoub M. Valve-conserving operation for aortic root aneurysm or dissection. Oper Tech Card Thorac Surg. 1996;1(1):57-67.
- David TE. Remodeling the aortic root and preservation of the native aortic valve. Oper Tech Card Thorac Surg. 1996;1(1):44-56.
- Aoyagi S, Kosuga K, Akashi H, Oryoji A, Oishi K. Aortic root replacement with a composite graft: results of 69 operations in 66 patients. Ann Thorac Surg. 1994;58(5):1469-1475.
- Vecsey-Nagy M, Jermendy Á, Szabó G, et al. Bilateral coronary ostial stenosis after Bentall procedure in a patient with Marfan syndrome. J Cardiovasc Emerg. 2018;3(4):193-196.
- Dossche KM, Tan ME, Schepens MA, Morshuis WJ, de la Rivière AB. Twenty-four year experience with reoperations after ascending aortic or aortic root replacement. Eur J Cardiothorac Surg. 1999;16(6):607-612.
- Malvindi PG, Cappai A, Raffa GM, et al. Analysis of postsurgical aortic false aneurysm in 27 patients. Tex Heart Inst J. 2013;40(3):274-280.
- Dougenis D, Daily BB, Kouchoukos NT. Reoperations on the aortic root and ascending aorta. Ann Thorac Surg. 1997;64(4):986-992.
- Rankin JS. An interrupted suture technique for ascending aortic replacement concomitant to aortic valve repair. J Heart Valve Dis. 2012;21(2):263-266.
Acknowledgements
The author would like to thank Saad A. Khan and Zabreen Ahmed for the video narration.



