
ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Treating Intractable Hiccups by Clipping the Phrenic Nerve Using VATS
Felipe Torres España N, Ramirez Pereira J, Felipe Aristizábal López C, Alejandra Gil M. Treating Intractable Hiccups by Clipping the Phrenic Nerve Using VATS. February 2025. doi:10.25373/ctsnet.28485989
Clinical Case
A 46-year-old male with HIV and a history of gastroesophageal reflux disease currently being treated with Dolutegravir started experiencing intermittent hiccups eight months prior to this procedure. During the previous four months, the hiccups became persistent, occurring approximately 4-6 times per hour, significantly impacting his quality of life.
The patient tried various treatments, including proton pump inhibitors, Metoclopramide, Baclofen, and alternative treatments such as acupuncture, but none resulted in improvement.
He consulted a thoracic surgery service in Bogotá, Colombia, where some initial tests were ordered, including a diaphragm fluoroscopy. This revealed significant elevation of both hemidiaphragms during hiccup episodes. Based on this, his treating doctor recommended clipping the phrenic nerve to improve his quality of life.
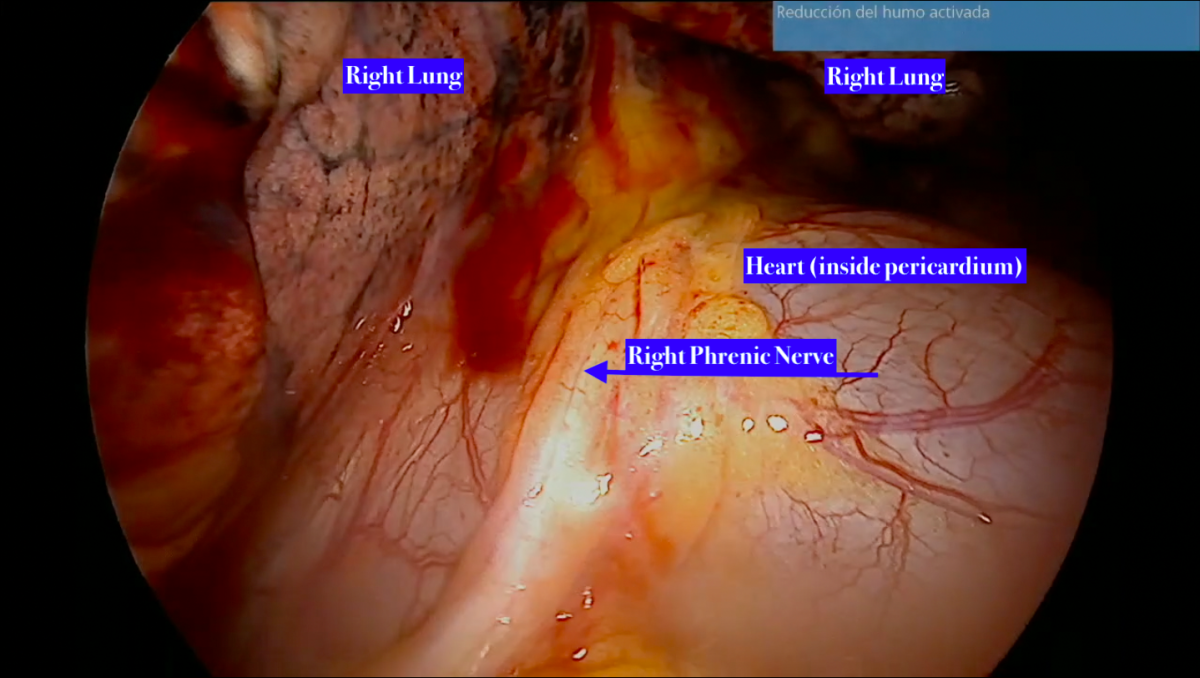
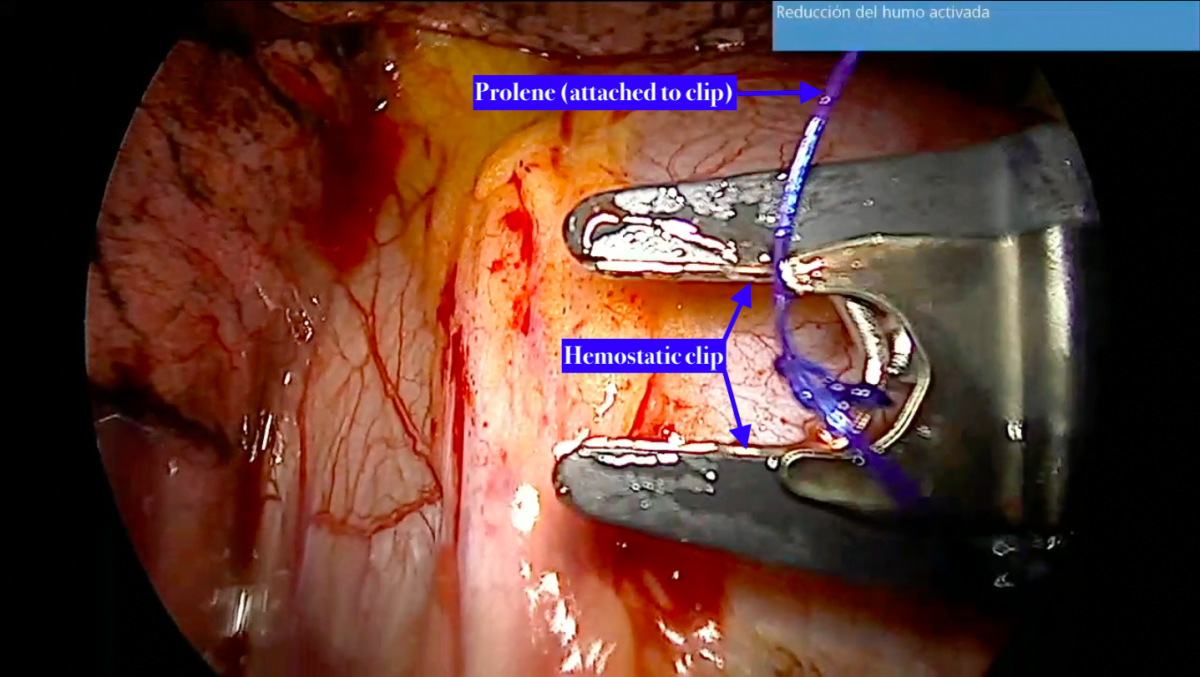
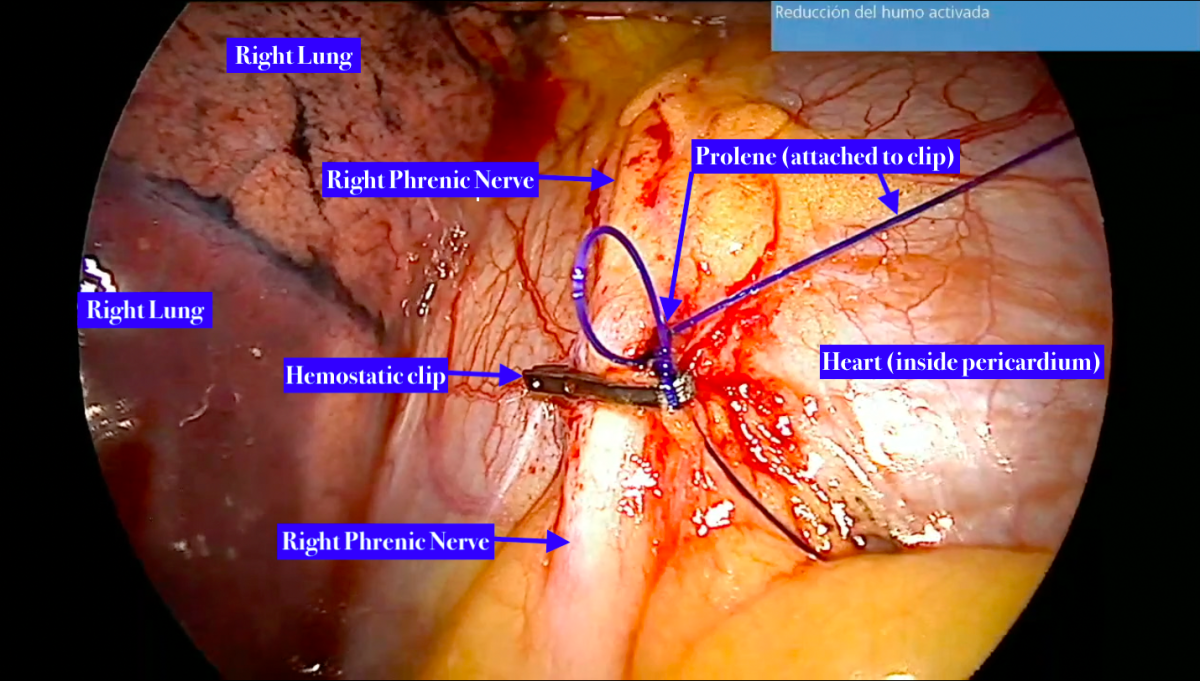
Clipping the phrenic nerve was temporary, which reduces the risk of diaphragm paralysis. The temporary clip was made of Prolene and removed 10 days after surgery.
Within the first month of postoperative follow-up, the patient showed no recurrence of hiccup episodes. He continues to attend follow-up appointments and has not experienced any new episodes of hiccups.
Disclaimer
The information and views presented on CTSNet.org represent the views of the authors and contributors of the material and not of CTSNet. Please review our full disclaimer page here.




Comments